1. Introduction
It is reported that there are 120–180 million hepatitis C virus (HCV) carriers around the world, with the worldwide prevalence estimated at 3% (Shepard et al.,
2005; Tong et al.,
2012). Chronic hepatitis C is considered to be a major cause of liver disease, including progressive liver fibrosis, cirrhosis, and hepatocellular carcinoma (Hoofnagle,
2002; Shepard et al.,
2005; Thomas and Seeff,
2005; Micallef et al.,
2006; Zhu et al.,
2014). The risk factors like older age, consumption of alcohol, metabolic alterations, liver necroinflammation, duration of infection and viral co-infections (Poynard et al.,
2003), and insulin resistance (Romero-Gómez et al.,
2005) can influence the degree of liver fibrosis. More and more evidence also shows that vitamin D status is very important for the liver disease severity in patients who are infected with chronic hepatitis C (Terrier et al.,
2012; Kitson et al.,
2013; Ladero et al.,
2013; Lange et al.,
2013). 25-Hydroxyvitamin D or 25(OH) D is a metabolite of vitamin D in liver, and is exported to combine with vitamin D binding protein (VDBP). Because the half-life of serum 25(OH) D is long, the serum concentration of 25(OH) D is the most commonly used biomarker for vitamin D status (Wang et al.,
2004; Stokes et al.,
2013). Vitamin D plays an important role not only in maintenance of skeletal health, but also in the immune response, wound healing and many other important physiological functions (Cholongitas et al.,
2012). 1,25-Dihydroxyvitamin D also plays an important role for innate and adaptive immune pathways (von Essen et al.,
2010).
Recently, studies have reported that the 25(OH) D level decreased in patients with various forms of chronic liver disease and advanced fibrosis (Arteh et al.,
2010; Geier,
2011). A lower serum 25(OH) D level significantly correlates with an increasing risk of advanced fibrosis and a higher severity of necroinflammatory activity has been related to different populations with individuals infected with chronic hepatitis C (Lange et al.,
2011;
2013; Kitson et al.,
2013; Petta et al.,
2013). However, the results are not consistent in different studies and by race (Kitson et al.,
2013; White et al.,
2013). Taking into account that a single study may have been insufficient to detect the overall effects that vitamin D can have on populations with different genetic backgrounds, the accumulated data from different studies and quantitative synthesis were thought to be very important in providing evidence of the association of serum vitamin D levels and the severity of liver fibrosis in the patients who are infected with HCV. So, we carried out this meta-analysis on all published studies to estimate the overall effects of serum vitamin D levels and the severity of liver fibrosis. The heterogeneity between the individual studies and the potential publication bias was also evaluated. This meta-analysis is different from that reported by Villar et al. (
2013), which focused on the association between 25(OH) D and sustained virological response (SVR) in HCV-infected individuals.
2. Materials and methods
2.1. Literature search strategy
We conducted a literature search of available materials prior to October 2013 in the PubMed and EMBASE databases without restrictions. The search items were “vitamin D or 25(OH) D” and “HCV or chronic hepatitis C or chronic liver disease”. The search results also included articles reviewed ahead of publication. Moreover, the references cited by the selected articles and published reviews were scanned for additional relevant studies. We also contacted the authors for additional information if necessary.
2.2. Eligibility criteria
Studies were included in the meta-analysis if they met the following standards: (1) the association between the severity of liver fibrosis and the blood (plasma or serum) vitamin D or 25(OH) D status was evaluated; (2) the results showed interest and relevance to the fibrosis stage of the patients infected with HCV; (3) the results provided the odds ratio (OR) with 95% confidence intervals (CIs) or a mean with standard deviation (SD) or adequate information to calculate them. Abstracts, conference proceedings, case reports, reviews, patients co-infected with HIV, and repeated literatures were excluded. The most complete studies were those selected in which there were several studies available from the same investigators.
2.3. Data extraction
All data from the included studies were independently extracted by two authors. Any disagreements were resolved by discussions according to the selection criteria guidelines. Finally, the data for this meta-analysis were made available from six studies. The following data were extracted: name of the first author, publication year, ethnic background, participant sex and age, sample size (cases and controls or group size), fibrosis stage, measure of vitamin D, OR estimates with 95% CIs, or mean with SD (all of the data are shown in Table
1).
Table 1
Characteristics of studies on serum vitamin D status and severity of liver fibrosis
| Source |
Ethnic background |
Study |
Sex |
Age (year)1
|
n
c
|
n
p
|
Study quality2
|
Measure of vitamin D |
| Petta et al., 2013
|
Italy |
Consecutive |
M/F |
52.8±11.9 |
74 |
260 |
7 |
Chromosystem reagent and HPLC |
| Lange et al., 2011
|
Germany |
Retrospective |
M/F |
45 (22–72) |
146 |
6567 |
6 |
Radioimmunoassay |
| Arteh et al., 2010
|
55% Caucasian, 45% African American |
Consecutive |
M/F |
53±9 |
43 |
118 |
6 |
Automated chemiluminescence immunoassay |
| White et al., 2013
|
African |
Cross-sectional |
M |
57.4±4.2 |
63 |
289 |
6 |
Automated immunochemiluminometric assay |
| American White (non-Hispanic) |
55.7±5.5 |
54 |
6 |
Automated immunochemiluminometric assay |
| Kitson et al., 2013
|
Caucasian |
CHARIOT |
M/F |
43.9±9.4 |
44 |
896 |
7 |
LC-MS/MS methodology |
| Amanzada et al., 2013
|
Germany (Caucasian) |
Cohort |
M/F |
51±10 |
36 |
191 |
6 |
Chromatographic system and HPLC |
|
|
| Source |
OR/relative risk (95% CI) |
Mean (95% CI) |
HCV type |
How fibrosis assessed and diagnosis criteria |
Severe fibrosis vs. zero or lesser degrees |
|
| Petta et al., 2013
|
0.958 (0.919, 0.999) |
−0.44 (−0.71, −0.16) |
G1 |
Biopsy according to Scheuer numerical scoring system |
F3–F4 vs. F0–F1 |
| Lange et al., 2011
|
0.74 (0.548, 1.000) |
|
G1, 2, 3 |
Biopsy according to METAVIR model |
F2–F4 vs. F0–F1 |
| Arteh et al., 2010
|
0.681 (0.377, 1.229) |
|
NA |
By liver biopsy or by clinical or biochemical evidence of hepatocellular failure and/or portal hypertension |
Cirrhosis vs. without cirrhosis |
| White et al., 2013
|
12.91 (1.30, 128.16) |
|
G1, 2, 3, 4 |
By biochemical evidence according to FibroSURE-ActiTest model |
F3/F4–F4 vs. F0–F3 |
| 0.84 (0.20, 3.59) |
| Kitson et al., 2013
|
|
−0.21 (−0.53, 0.12) |
G1 |
Liver biopsy according to METAVIR model |
F3/F4 vs. F0–F2 |
| Amanzada et al., 2013
|
|
−0.80 (−1.10, −0.50) |
G1 |
Liver specimens, NA |
Severe fibrosis/cirrhosis vs. absent/mild/moderate |
1Data are expressed as mean±SD or mean (range)
2Study quality was judged on the basis of the Newcastle-Ottawa scale (1–9 stars)
n
c: number of cases; n
p: number of participants; M: male; F: female; CHARIOT: collaborative group hepatitis C study using high-dose Pegasys RBV induction dose in genotype one; HPLC: high performance liquid chromatography; LC: liquid chromatography; MS: mass spectrometry; G1, 2, 3, 4: hepatitis C genotype 1, 2, 3, or 4 infection; NA: not available
2.4. Statistical analysis
We quantified the relationship between serum vitamin D status and severity of liver fibrosis in chronic hepatitis C patients by using a random-effects model, which considered variation both within and between the studies. Sensitivity analysis was performed by deleting each study which reflected the influence of the individual dataset on the pooled ORs. Subgroup analysis was performed by geographic region and ethnic background. An estimation of potential publication bias was assessed by using Egger’s linear regression test (Egger et al.,
1997). All statistical tests were performed with the STATA software 12.0.
P<0.05 was considered statistically significant.
3. Results
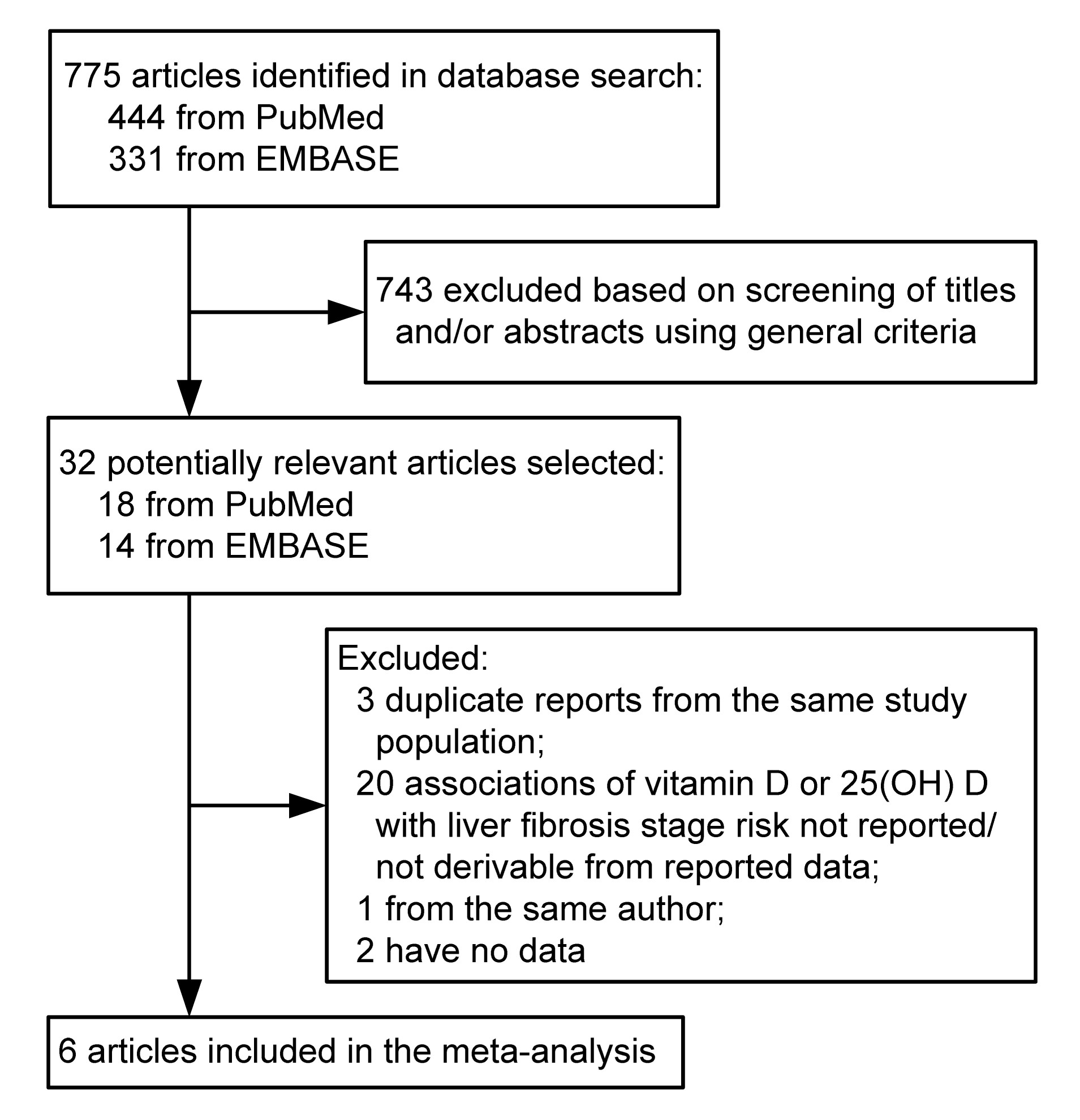
3.1. Literature search
A flow diagram of our literature search is shown in Fig.
1. Our total search yielded 775 entries. We identified six eligible publications (Arteh et al.,
2010; Lange et al.,
2011; Amanzada et al.,
2013; Kitson et al.,
2013; Petta et al.,
2013; White et al.,
2013) concerning the association between vitamin D and severity of liver fibrosis in patients infected with chronic hepatitis C. Among these studies, two (Arteh et al.,
2010; Petta et al.,
2013) were consecutive studies, one (Lange et al.,
2011) was a retrospective study, one (White et al.,
2013) was a cross-sectional study, one (Kitson et al.,
2013) was a CHARIOT study, and one was a cohort study (Amanzada et al.,
2013).
Fig.1
Flowchart of the literature search
3.2. Study characteristics
The six studies concerning the relationship between serum vitamin D and the severity of liver fibrosis were published between 2010 and 2013 (Table
1), which involved a total of 8321 patients. Of these six studies, three (Lange et al.,
2011; Amanzada et al.,
2013; Petta et al.,
2013) were conducted in Europe, two (Arteh et al.,
2010; White et al.,
2013) in the United States, and one (Kitson et al.,
2013) in Australia. The five (Arteh et al.,
2010; Amanzada et al.,
2013; Kitson et al.,
2013; Petta et al.,
2013; White et al.,
2013) studies assessed included a review of serum 25(OH) D status, and one (Lange et al.,
2011) on 25(OH)D
3 and 1,25(OH)
2D
3 status. Three studies (Amanzada et al.,
2013; Kitson et al.,
2013; Petta et al.,
2013) included patients with chronic hepatitis C genotype 1 infection, one (Lange et al.,
2011) with chronic hepatitis C genotype 1, 2, or 3-infection, one (White et al.,
2013) with chronic hepatitis C genotype 1, 2, 3, or 4-infection, and one (Arteh et al.,
2010) did not specify the kind of HCV type. Four studies (Baur et al.,
2012; Corey et al.,
2012; Weintraub et al.,
2012; Ladero et al.,
2013) were excluded because they did not report usable data. One study (Petta et al.,
2010) was excluded because it reported on the same author.
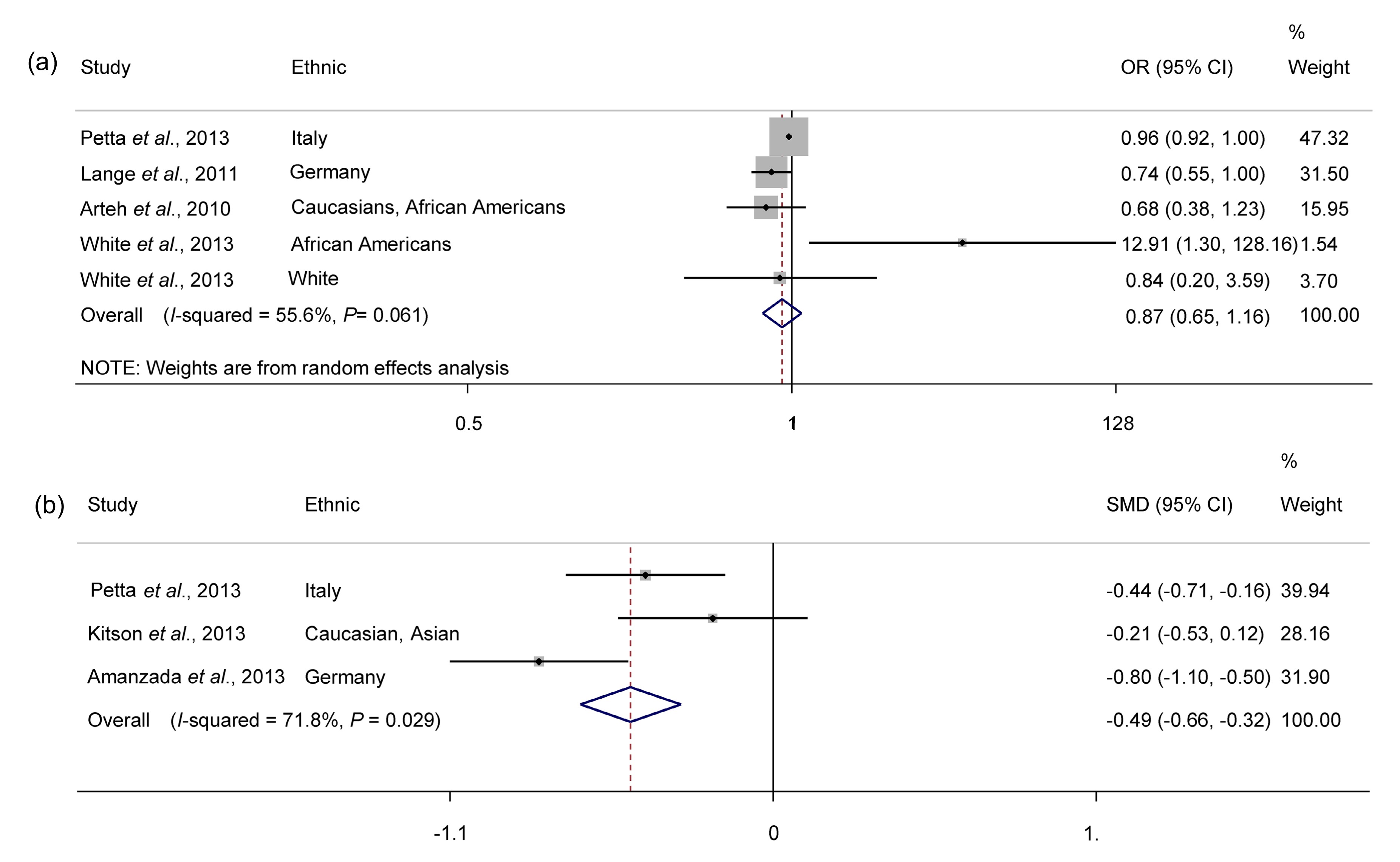
3.3. Serum vitamin D status and severity of liver fibrosis
The overall results for the serum vitamin D status associated with the severity of liver fibrosis are shown in Fig.
2. Results from studies concerning the relationship between serum vitamin D status and severity of liver fibrosis were inconsistent with inverse or positive associations reported. The pooled OR was 0.866 (95% CI, 0.649 to 1.157) and mean was −0.487 (95% CI, −0.659 to −0.315). There was statistically significant heterogeneity among mean data extracted studies (
P=0.029;
I
2=71.8%) but not among OR data extracted studies (
P=0.061;
I
2=55.6%).
Fig.2
Forest plot of serum vitamin D status and severity of liver fibrosis
(a) Pooled OR; (b) Pooled mean
3.4. Stratifying analysis
Stratifying by geographic region, the pooled ORs of studies were 1.33 (95% CI, 0.35 to 5.08;
P=0.052;
I
2=66.2%) for studies conducted in the United States, and 0.88 (95% CI, 0.694 to 1.116;
P=0.096;
I
2=64.0%) for studies conducted in Europe. There was no statistically significant heterogeneity among the studies (United States,
P=0.052 and
P=0.096). Stratifying by ethnic background, the pooled ORs of studies were 0.902 (95% CI, 0.762 to 1.068;
P=0.246;
I
2=28.8%) for those with a European ethnic origin (Table
2). We did not do subgroup analysis about the mean data extracted studies because only three studies were included in our research (Amanzada et al.,
2013; Kitson et al.,
2013; Petta et al.,
2013).
Table 2
Association between serum vitamin D status and severity of liver fibrosis stratified according to geographic region and ethnic background
| Factor |
RR |
95% CI |
Heterogeneity
|
|
P
|
I
2 (%) |
| Geographic region |
| United States |
1.33 |
0.35–5.08 |
0.052 |
66.2 |
| Europe |
0.88 |
0.694–1.116 |
0.096 |
64.0 |
| Ethnic background |
| European |
0.902 |
0.762–1.068 |
0.246 |
28.8 |
RR: relative risk; CI: confidence interval
3.5. Sensitivity analysis and publication bias
We performed sensitivity analysis by omitting one study at a time and calculating the pooled OR for the remainder of the studies. The result showed that the study of White et al. (
2013) influenced the pooled OR. After excluding this single study, the heterogeneity was significantly reduced (
P=0.246;
I
2=28.8%; 95% CI, 0.762 to 1.068). The Egger’s test showed no evidence of publication bias for OR (
P=0.902) or mean (
P=0.888) data extracted studies.
4. Discussion
Vitamin D deficiency is a global problem. There are 20% to 100% of people suffering from this problem when referring to serum vitamin D concentrations <20 ng/ml (Holick et al.,
2011). Low vitamin D status associated with advanced fibrosis in chronic hepatitis C patients (Arteh et al.,
2010; Geier,
2011) has been reported. The reasons why vitamin D deficiency occurs in chronic hepatitis C patients are far from conclusive. A possible reason of this finding should consider the multiple interconnections among vitamin D, the immune response, and inflammatory status (Baeke et al.,
2010; Hewison,
2010).
The current meta-analysis summarizes the results of group studies, including six studies and a total of 8321 participants. The findings from the mean data extracted studies indicated that serum vitamin D status is inversely associated with the severity of liver fibrosis, but the results from the OR data extracted studies showed that there was no significant association between serum vitamin D status and the severity of liver fibrosis. When the analysis was stratified according to geographic region and ethnic background, the results were unchanged. However, after excluding the study of White et al. (
2013), the heterogeneity was significantly reduced.
White et al. (
2013) found that serum levels of vitamin D (>50 ng/ml) have a higher risk of advanced fibrosis (F3/F4–F4) in African American males. Corey et al. (
2012) found that African Americans whose liver fibrosis clinically progressed over a 4-year period had higher baseline vitamin D levels compared with African Americans whose fibrosis had not progressed (32.7 ng/ml vs. 25.2 ng/ml;
P=0.08). These different results may be due to the different vitamin D measurements, study design, or skin tone. It has been reported that very few foods naturally contain vitamin D and the major cause of vitamin D deficiency is due to the inadequate exposure to sunlight (Holick et al.,
2007; Holick and Chen,
2008). People with a naturally dark skin tone have natural sun protection and require three to five times longer exposure to make the same amount of vitamin D as a person with a white skin tone (Clemens et al.,
1982; Hintzpeter et al.,
2008).
The findings from this meta-analysis need to be confirmed in large randomized clinical trials. Some suggestions should be considered in further studies. First, most of the studies included were conducted in America and Europe. Even more studies should be conducted in other populations such as South-African and Asian, considering the underlying disease-effect unconformity across different geographical locations. Second, more accurate questionnaires or other accurate methods assessing serum vitamin D status could provide better results for estimating the association.
Several limitations of this study should be addressed. First, meta-analyses are considered hypothesis-generating. The quality and usefulness of any meta-analysis are dependent on the quality and comparability of data from the component studies (Hennekens and Demets,
2009). Inadequate or inaccurate data may bias the results. And unknown confounding cannot be excluded as a potential explanation for the observed findings. Second, the related data on serum vitamin D concentration were measured by different methods. This may possibly lead to less accurate estimates of risk. Meanwhile, only six studies were available for this study, some of the subgroup analyses were difficult to perform. Third, although there was a lack of any indication of major publication bias in the formal evaluation we used, potential publication bias is impossible to completely exclude because some studies with null results tend not to be published. Finally, There was significant heterogeneity for mean data extracted studies (
I
2=71.8%) in the pooled analysis. This may be due to the different serum vitamin D concentration detection, different ethnic backgrounds included, different fibrosis assessing models, or other confounding factors which have not been considered.
In summary, although data from the mean data extracted studies suggest that lower serum vitamin D is a risk factor for severity of liver fibrosis, there is no conclusive evidence on this association because of inconsistencies between OR data extracted studies and mean data extracted studies. Prospective studies focusing on more detailed results, including more accurate vitamin D measurement technology, and taking a broad range of confounders into account are required to clarify this relationship.
* Project supported by the National Science and Technology Major Project of the Ministry of Science and Technology of China (No. 2012ZX10002006), the Key Technologies R&D Program of Zhejiang Province (No. 2012C03SA170003), and the Hangzhou Key Technologies R&D Program (No. 20122513A49), ChinaCompliance with ethics guidelines Yue-qiu LUO, Xiao-xing WU, Zong-xin LING, Yi-wen CHENG, Li YUAN, and Charlie XIANG declare that they have no conflict of interest.References
[1] Amanzada, A., Goralczyk, A.D., Moriconi, F., 2013. Vitamin D status and serum ferritin concentration in chronic hepatitis C virus type 1 infection.
J Med Virol, 85(9):1534-1541.


[2] Arteh, J., Narra, S., Nair, S., 2010. Prevalence of vitamin D deficiency in chronic liver disease.
Dig Dis Sci, 55(9):2624-2628.
[3] Baeke, F., Takiishi, T., Korf, H., 2010. Vitamin D: modulator of the immune system.
Curr Opin Pharmacol, 10(4):482-496.
[4] Baur, K., Mertens, J.C., Schmitt, J., 2012. Combined effect of 25-OH vitamin D plasma levels and genetic V
itamin D R
eceptor (NR 1I1) variants on fibrosis progression rate in HCV patients.
Liver Int, 32(4):635-643.
[5] Cholongitas, E., Theocharidou, E., Goulis, J., 2012. Review article: the extra-skeletal effects of vitamin D in chronic hepatitis C infection.
Alimen Pharmacol Ther, 35(6):634-646.
[6] Clemens, T.L., Henderson, S.L., Adams, J.S., 1982. Increased skin pigment reduces the capacity of skin to synthesise vitamin D
3
.
Lancet, 319(8263):74-76.
[7] Corey, K.E., Zheng, H., Mendez-Navarro, J., 2012. Serum vitamin D levels are not predictive of the progression of chronic liver disease in hepatitis C patients with advanced fibrosis.
PLoS ONE, 7(2):e27144
[8] Egger, M., Davey, S.G., Schneider, M., 1997. Bias in meta-analysis detected by a simple, graphical test.
BMJ, 315(7109):629-634.
[9] Geier, A., 2011. Shedding new light on vitamin D and fatty liver disease.
J Hepatol, 55(2):273
[10] Hennekens, C.H., Demets, D., 2009. The need for large-scale randomized evidence without undue emphasis on small trials, meta-analyses, or subgroup analyses.
JAMA, 302(21):2361-2362.
[11] Hewison, M., 2010. Vitamin D and the intracrinology of innate immunity.
Mol Cell Endocrinol, 321(2):103-111.
[12] Hintzpeter, B., Scheidt-Nave, C., Mller, M.J., 2008. Higher prevalence of vitamin D deficiency is associated with immigrant background among children and adolescents in Germany.
J Nutr, 138(8):1482-1490.
[13] Holick, M.F., Chen, T.C., 2008. Vitamin D deficiency: a worldwide problem with health consequences.
Am J Clin Nutr, 87(4):1080S-1086S.
[14] Holick, M.F., Chen, T.C., Lu, Z., 2007. Vitamin D and skin physiology: a D-lightful story.
J Bone Miner Res, 22(Suppl. 2):V28-V33.
[15] Holick, M.F., Binkley, N.C., Bischoff-Ferrari, H.A., 2011. Evaluation, treatment, and prevention of vitamin D deficiency: an endocrine society clinical practice guideline.
J Clin Endocrinol Metab, 96(7):1911-1930.
[16] Hoofnagle, J.H., 2002. Course and outcome of hepatitis C.
Hepatology, 36(5 Suppl. 1):S21-S29.
[17] Kitson, M.T., Dore, G.J., George, J., 2013. Vitamin D status does not predict sustained virologic response or fibrosis stage in chronic hepatitis C genotype 1 infection.
J Hepatol, 58(3):467-472.
[18] Ladero, J.M., Torrejn, M.J., Snchez-Pobre, P., 2013. Vitamin D deficiency and vitamin D therapy in chronic hepatitis C.
Ann Hepatol, 12(2):199-204.
[19] Lange, C.M., Bojunga, J., Ramos-Lopez, E., 2011. Vitamin D deficiency and a CYP27B1-1260 promoter polymorphism are associated with chronic hepatitis C and poor response to interferon-alfa based therapy.
J Hepatol, 54(5):887-893.
[20] Lange, C.M., Miki, D., Ochi, H., 2013. Genetic analyses reveal a role for vitamin D insufficiency in HCV-associated hepatocellular carcinoma development.
PLoS ONE, 8(5):e64053
[21] Micallef, J.M., Kaldor, J.M., Dore, G.J., 2006. Spontaneous viral clearance following acute hepatitis C infection: a systematic review of longitudinal studies.
J Viral Hepat, 13(1):34-41.
[22] Petta, S., Camm, C., Scazzone, C., 2010. Low vitamin D serum level is related to severe fibrosis and low responsiveness to interferon-based therapy in genotype 1 chronic hepatitis C.
Hepatology, 51(4):1158-1167.
[23] Petta, S., Grimaudo, S., Marco, V.D., 2013. Association of vitamin D serum levels and its common genetic determinants, with severity of liver fibrosis in genotype 1 chronic hepatitis C patients.
J Viral Hepatitis, 20(7):486-493.
[24] Poynard, T., Yuen, M.F., Ratzin, V., 2003. Viral hepatitis C.
Lancet, 362(9401):2095-2100.
[25] Romero-Gmez, M., Viloria, M.D.M., Andrade, R.J., 2005. Insulin resistance impairs sustained response rate to peginterferon plus ribavirin in chronic hepatitis C patients.
Gastroenterology, 128(3):636-641.
[26] Shepard, C.W., Finelli, L., Alter, M.J., 2005. Global epidemiology of hepatitis C virus infection.
Lancet Infect Dis, 5(9):558-567.
[27] Stokes, C.S., Volmer, D.A., Grnhage, F., 2013. Vitamin D in chronic liver disease.
Liver Int, 33(3):338-352.
[28] Terrier, B., Jehan, F., Munteanu, M., 2012. Low 25-hydroxyvitamin D serum levels correlate with the presence of extra-hepatic manifestations in chronic hepatitis C virus infection.
Rheumatology, 51(11):2083-2090.
[29] Thomas, D.L., Seeff, L.B., 2005. Natural history of hepatitis C.
Clin Liver Dis, 9(3):383-398.
[30] Tong, J., Wang, Y.W., Lu, Y.A., 2012. New developments in small molecular compounds for anti-hepatitis C virus (HCV) therapy.
J Zhejiang Univ-Sci B (Biomed & Biotechnol), 13(1):56-82.
[31] Villar, L.M., Del Campo, J.A., Ranchal, I., 2013. Association between vitamin D and hepatitis C virus infection: a meta-analysis.
World J Gastroenterol, 19(35):5917
[32] von Essen, M.R., Kongsbak, M., Schjerling, P., 2010. Vitamin D controls T cell antigen receptor signaling and activation of human T cells.
Nat Immunol, 11(4):344-349.
[33] Wang, T.T., Nestel, F.P., Bourdeau, V., 2004. Cutting edge: 1,25-dihydroxyvitamin D
3 is a direct inducer of antimicrobial peptide gene expression.
J Immunol, 173(5):2909-2912.
[34] Weintraub, S.J., Fleckenstein, J.F., Marion, T.N., 2012. Vitamin D and the racial difference in the genotype 1 chronic hepatitis C treatment response.
Am J Clin Nutr, 96(5):1025-1031.
[35] White, D.L., Tavakoli-Tabasi, S., Kanwal, F., 2013. The association between serological and dietary vitamin D levels and hepatitis C-related liver disease risk differs in African American and white males.
Aliment Pharmacol Ther, 38(1):28-37.
[36] Zhu, Y., Zheng, Y., Shen, Y.Y., 2014. Analyzing and modeling rheological behavior of liver fibrosis in rats using shear viscoelastic moduli.
J Zhejiang Univ-Sci B (Biomed & Biotechnol), 15(4):375-381.

Open peer comments: Debate/Discuss/Question/Opinion
<1>