1. Introduction
Pulmonary embolism (PE) is defined as the blockage of the main pulmonary artery or its branches by substances that have travelled through the bloodstream, most commonly resulting from deep-vein thrombosis (DVT). It occurs in more than 0.6 million people in the United States each year (Rahimtoola and Bergin,
2005), with a mortality of 0.5 to 2 million per year. The chief symptoms of PE include breathlessness, chest pain on inspiration, and palpitations (Kumar,
2010). Clinical signs include low blood oxygen saturation (also known as hypoxemia) and cyanosis, rapid breathing rate, and a rapid heart rate. Severe cases of PE can lead to syncope, abnormally low blood pressure, and sudden death (Goldhaber,
2005). The risk of PE increases in various situations, such as postoperative or long-term bedridden patients. Diagnosis is based on these clinical findings in combination with laboratory tests (such as the D-dimer tests) and imaging studies, usually a computed tomography (CT) pulmonary angiography (Goldhaber,
2005). Diagnosis of PE is usually underestimated due to the limited diagnostic tools in the past. However, with state-of-the-art technologies, the recognition of PE is gradually increasing in modern China (Yang et al.,
2011).
Coexistence of PE and arterial thrombosis in a single individual is rare around the world (Wang,
2012). The more commonly reported situations are patients with potential arteriovenous shunts, such as patent foramen ovale (PFO), atrial septal defect (ASD), or pulmonary arteriovenous fistula (PAVF). Embolus may enter the systemic circulation from the right heart system, as the term of a paradoxical embolism (Rakhit,
2003). It is extremely rare but can happen in a PE concurrent with systemic embolism in conditions of cancer, antiphospholipid syndrome, or other hypercoagulable states. Treatment of PE is typically handled with anticoagulant medications, including heparin and warfarin. Severe cases may require intravenous thrombolysis using medication such as tissue plasminogen activator, or ask for a surgical intervention with pulmonary thrombectomy (Goldhaber,
2005). However, for patients with arteriovenous thrombosis, both antiplatelet and anticoagulation therapy should be adopted simultaneously. A careful evaluation of both the ischemic and hemorrhagic risks is required to achieve the maximum clinical benefit. Herein, we present an unusual case of acute myocardial infarction (AMI) and cerebral infarction secondary to acute PE with a planned follow-up for more than 16 months.
2. Case report
A 55-year-old woman was presented to the emergency room of the Second Affiliated Hospital, School of Medicine, Zhejiang University, China, complaining of chest distress and dyspnea for two days and then abrupt loss of consciousness for 1 h. Her husband also reported a 10-month history of recurrent shortness of breath and dizziness, for which she had been diagnosed as having “bronchitis” and was taking “aminophylline” and “Ginkgo Leaf”, but her symptoms had not been relieved. She also had a history of varicose veins of the lower extremities for 10 years. On physical examination, she was found to be tachycardic with 110 beats/min and her blood pressure was 130/92 mmHg, with cyanosis lip and varicose superficial veins at both lower extremities. A pulse oximetry with the patient at rest and breathing room air showed a low oxygen saturation of 89%. An electrocardiogram (ECG) demonstrated sinus tachycardia. Routine laboratory studies revealed a mild hypoxemia with 62.4 mmHg of the oxygen pressure and hyperventilation with 23.9 mmHg of the carbon dioxide pressure, which indicated respiratory alkalosis. The serum creatinine kinase level was normal, but the level of troponin-I mildly elevated to 0.16 ng/ml (normal <0.06 ng/ml). The serum D-dimer level moderately increased to 770 μg/L (normal <330 μg/L).
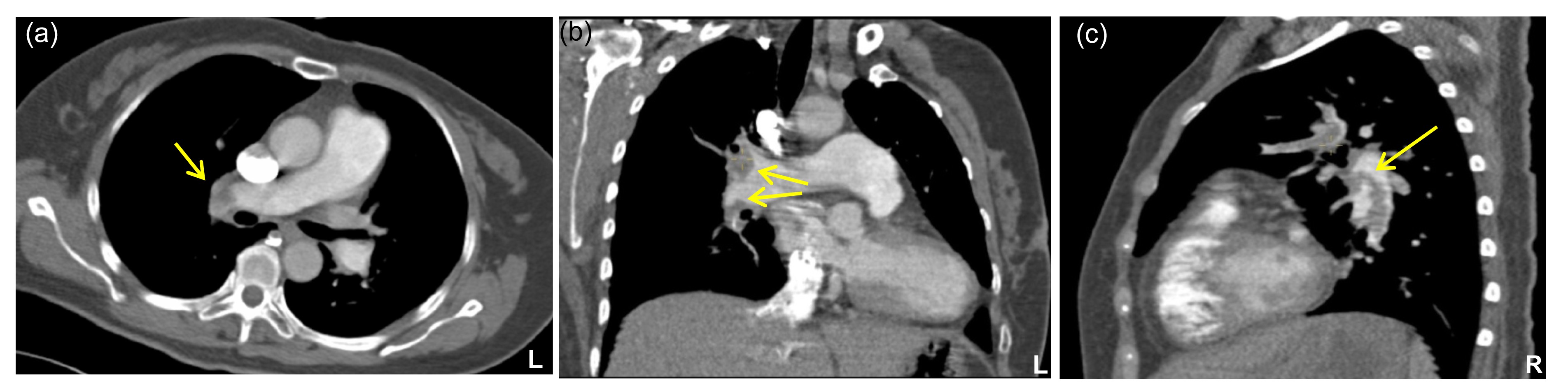
The patient restored to consciousness shortly after arrived in the emergency room. No lesion was found in the head through a CT scan, with only a slight inflammatory effusion in the inferior lobes of the bilateral lungs. After staying in the emergency room for 3 h, the patient’s face suddenly turned into pale and clammy, accompanied with her blood pressure decreasing to 69/45 mmHg and heart rate to 59 beats/min. A CT pulmonary angiography showed a massive PE in the right main pulmonary artery and both pulmonary arterial branches (Fig.
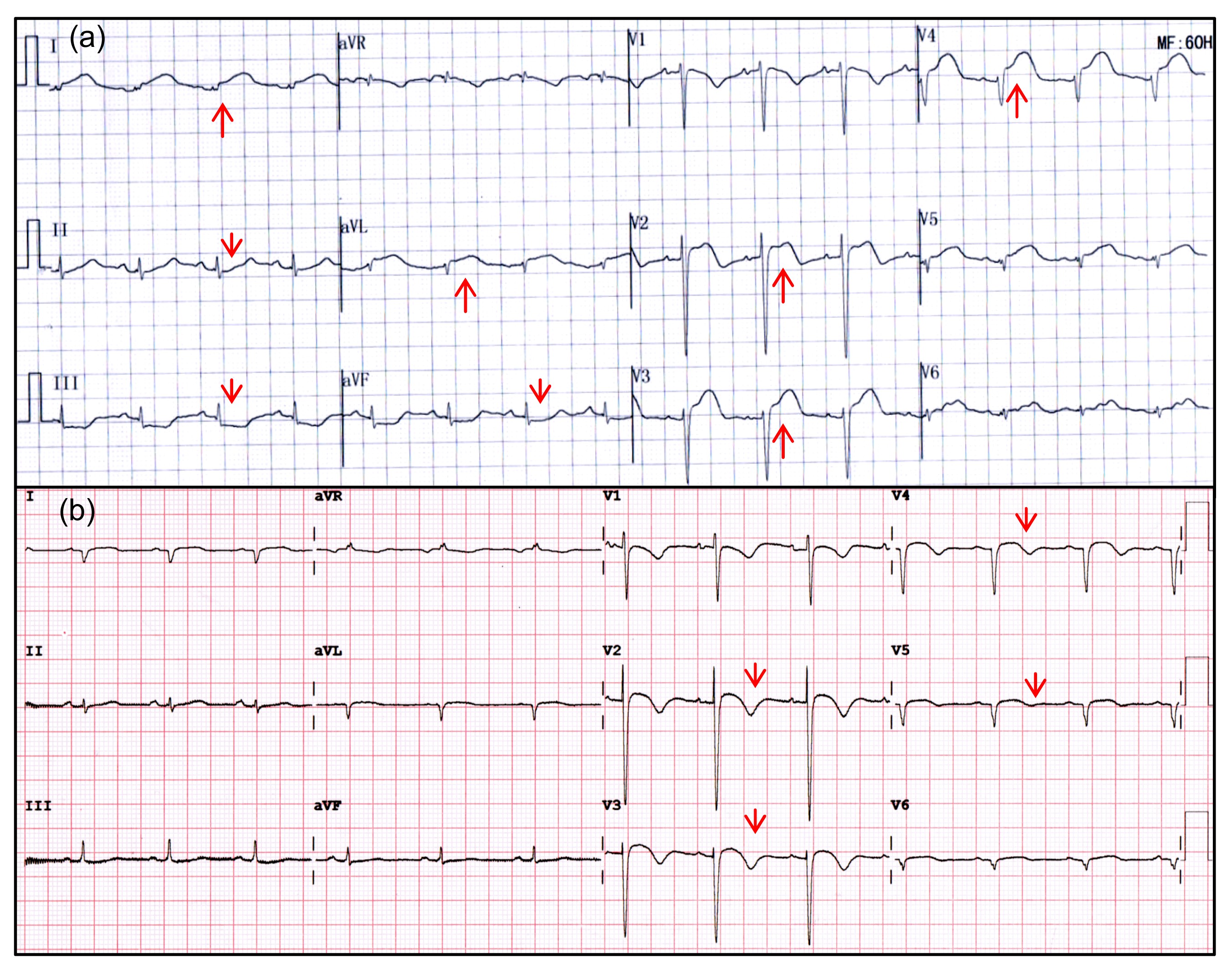
1). An ECG indicated a sinus rhythm with a dome-shaped ST-segment elevation in leads I, avL, V2 to V4 and opposite depression in leads II, III, avF (Fig.
2a). The progression of the R waves in precordial leads as V3 to V6 was poor (Fig.
2a). A regional left ventricular wall motion abnormality (RWMA) in the anterior and septal walls and 48% of the left ventricular ejection fraction (LVEF) were found through an echocardiogram (Fig.
3a). After consulting with a pneumologist and cardiologist, intravenous administration of 150 million units of urokinase was infused within 2 h and a dual antiplatelet therapy with aspirin and clopidogrel was orally administered at 300 mg, respectively. Four hours after thrombolysis, the serum D-dimer level was reduced to 20 μg/L, but the serum troponin-I elevated to 150.5 ng/ml. The elevated ST-segment in leads I, avL, V2 to V4 fell down to the baseline, and the T wave inversion was found in the precordial leads of V2 to V5 during the next 16 months (Fig.
2b). Subsequently, a low molecular weight heparin (LMWH) was injected subcutaneously every 12 h after 6 h of thrombolysis. The patient was then transferred to the coronary care unit (CCU) 12 h after thrombolysis, with serum D-dimer of 2723 μg/L and serum troponin-I of 66.7 ng/ml.
Fig.1
CT pulmonary angiography showing large filling defects in the right main artery and both pulmonary arterial branches: (a) axial view; (b) coronal view; (c) sagittal view
Contrast (bright white) seen in the main pulmonary artery and proximal left pulmonary arteries indicates patency; abrupt cut-off (lack of contrast; gray area) in both pulmonary arterial branches indicates thrombus as shown by arrows
Fig.2
Electrocardiogram examinations at the admission (a) and at the 16-month follow-up (b)
(a) A sinus rhythm with a dome-shaped ST-segment elevation in leads I, avL, V2 to V4 and opposite depression in leads II, III, avF were indicated. The progression of the R waves in precordial leads as V3 to V6 was poor. (b) The elevated ST-segment in leads I, avL, V2 to V4 fell down to the baseline, and the T waves inverted in the precordial leads of V2 to V5 during the next 16 months
Fig.3
Cardiac remodeling indicated by echocardiogram: (a) before the discharge and (b) at the 16-month follow-up
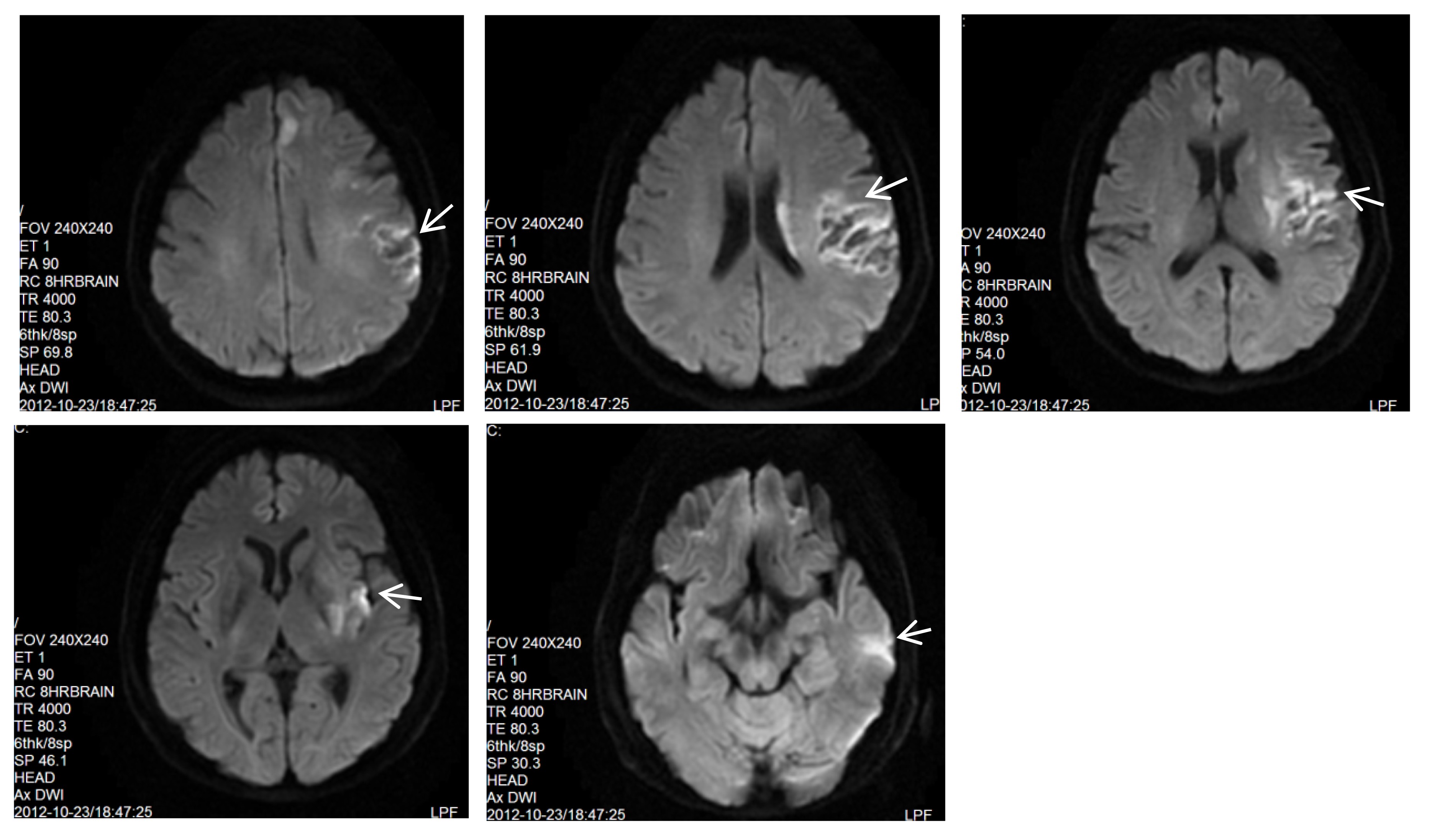
On Day 3 in the CCU, the patient complained of sudden non-fluent language and dyskinesis occurred at the right extremities. Physical examination revealed a motor aphasia, grade 0 muscle strength, and a positive Babinski’s sign at the right extremities. An urgent CT scan of the head showed a low density lesion in the left temporal and parietal lobes, which was diagnosed as an acute cerebral infarction. Neurology consultation suggested increasing the aspirin dosage to 200 mg daily on the basis of 75 mg clopidogrel per day orally and subcutaneous injection of 40 mg enoxaparin every 12 h, and a prescription of neuroprotective agents (ensign). Twenty-four hours after the onset of the acute stroke, a magnetic resonance imaging (MRI) examination of the head showed a recent infarction of the left temporal, parietal, insular lobes and basal ganglia, accompanied with partial hemorrhaging (Fig.
4). In the duration of the hospital stay, no thrombosis was found through a CT angiography, including the superficial, deep veins in the lower extremities, iliac veins, and inferior vena cava. Otherwise, ultrasonic inspection revealed no abnormal findings in the carotid, vertebral artery and upper extremity vessels, except for some stagnant blood flow in the right axillary vein. Coronary CT angiography showed a slight stenosis of the right coronary with an atherosclerotic lesion. CT pulmonary angiography ruled out pulmonary arteriovenous shunt and transoesophageal echocardiography excluded any cardiac shunts in this patient. Negative results were found in antinuclear antibody (ANA) screen with the anticardiolipin antibodies, tumor biomarkers, blood coagulation factors, other autoimmune antibodies and erythrocyte morphology.
Fig.4
Representative serial sections of head magnetic resonance imaging (MRI) by diffusion-weighted imaging (DWI) technique from parietal lobe to basis cranii
With the permission consent obtained, rivaroxaban was prescribed at a dosage of 10 mg twice daily instead of warfarin, and lower dosage of β-blocker clopidogrel and atorvastatin were also administered to prevent cardiovascular events. Before discharge, aphasia and dyskinesis in the patient’s right extremities were recovered, and blood flow of the right axillary vein and serum levels of D-dimer and troponin-I were normal. Pulmonary artery systolic pressure (PASP) evaluated by tricuspid valve regurgitation was monitored to follow up on the progression of PE through an echocardiogram, which showed a decline from 72 mmHg of the onset to 49 mmHg at the 1-month follow-up, and then to 26 mmHg at the 2-month follow-up. The RWMA phenomenon was still located at the anterior wall, and the LVEF was 57.9% evaluated through an echocardiogram. The CT pulmonary angiography at the 2-month follow-up revealed that a PE was primarily located at the lower right artery, with elimination in the main, bifurcation, and associated branches.
However, 10 months later, the patient came back to the clinics and complained of chest distress. Though the patient was taking anticoagulants, the PE had extended to the main portion of the right lower pulmonary artery, the right upper, and middle pulmonary arteries, and into the superior posterior segments of the left upper pulmonary artery. An echocardiogram showed myocardial thinning at the apex, middle to lower segment of the septum and anterior wall, with obvious RWMA. Cardiac insufficiency was indicated by the LVEF decreasing to 33% by the Simpson’s method, while the PASP elevated to 72 mmHg. Neither thrombus nor the reopening of the PFO can be detected by a transesophageal echocardiogram. The coronary angiography was also negative. According to the patient’s symptoms and examination, the anticoagulant was switched to warfarin. The international prothrombin time (PT) ratio was monitored regularly and targeted to 2.0–3.0.
The story seemed to be at an end. Six months later, the patient had an echocardiogram performed, which detected an apex aneurysm in left ventricle with enlargement of the left ventricle and both atriums (Fig.
3b). The cardiac index (LVEF) was slightly improved to 38% estimated by the Simpson’s method, and the PASP decreased to 54 mmHg. To attenuate the process of cardiac remodeling, a low dosage of angiotensin-converting enzyme inhibitor (perindopril) was prescribed.
3. Discussion
The morbidity of PE ranks third among all the cardiovascular diseases in the Western countries (Rahimtoola and Bergin,
2005). With the progression of diagnostic tools and knowledge update of this disease, the incidence of PE is increasing recently in China (Wang,
2010; Yang et al.,
2011). Patients with susceptible factors, such as postoperative, DVT, and long-term oral contraceptives, need to be alert to the complications of PE (Wang,
2012). Long-term bedridden patients, after arterial embolism, are prone to occurrences of PE. However, it is rare for the concurrent occurance of arterial embolism after PE, except for arteriovenous shunts and hypercoagulable disorders.
In the present case, the patient was first diagnosed as acute PE and subsequently found to have an acute myocardial and cerebral infarction. After an intravenous thrombolysis, serum cardiac enzymes elevated in a moderate-to-severe degree, and regional RWMA was found in the left ventricle, which was persistent until the 16 months’ follow-up examination after discharge. Although the patient was treated with the combination of anticoagulant, antiplatelet, atorvastatin, and β-blocker (Ying et al.,
2010), the cardiac remodeling was still ongoing, with cardiac chamber dilation and apex aneurysm formation. Various examinations did not support the possible existence of any arteriovenous shunts, a short reopening of the PFO, or hypercoagulable disorders. It may be explained that the increased right ventricular pressure and left ventricular RWMA after acute PE led to the formation of mural thrombus in the left ventricle, which would fall during thrombolysis and contribute to thromboembolism in the coronary and cerebral arteries. As a result, serum cardiac enzymes were dramatically elevated, which cannot be simply explained by the thrombolysis treatment. Chronic ventricular remodeling was another evidence to support either myocardial infarction or PE progression. During the progression of the disease, pulmonary embolus gradually shrunk in the 10 months’ follow-up examination, and then began to expand. As a result, the elevated pulmonary artery pressure could lead to an overweight afterload of the right ventricle, which aggravates the left ventricle remodeling through mechanical stretch and neuroendocrine mechanisms.
For half a century, the most commonly used medicine for PE patients was coumarin anticoagulants, such as warfarin (Zhang,
2012). This regimen is effective but complex for adjusting the PT to provide the right balance between the anticoagulation effect and hemorrhagic risk. Novel oral anticoagulants that are directed against the factor Xa or thrombin overcome some limitations of this standard therapy, including the need for injection and for regular dosage adjustments on the basis of laboratory monitoring. Rivaroxaban, a fixed-dose regimen of the oral factor Xa inhibitor, has been shown to be as effective as the standard anticoagulant therapy for the treatment of DVT (The EINSTEIN Investigators,
2010) and PE (The EINSTEIN-PE Investigators,
2012), without the need for laboratory monitoring. For patients with non-valvular atrial fibrillation, it has been found that rivaroxaban was non-inferior to warfarin for the prevention of stroke or systemic embolism, with no significance in the rate of major or non-major clinically relevant bleeding (Patel et al.,
2011). Recently, ATLAS-ACS2 TIMI 51 (an anti-Xa therapy to lower cardiovascular events in addition to standard therapy in subjects with acute coronary syndrome-thrombolysis in myocardial infarction 51) trial and associated meta-analysis were published, showing that rivaroxaban reduced the composite primary endpoint of cardiovascular death, myocardial infarction, and stroke. All-cause mortality in patients with a recent acute coronary syndrome was also attenuated in rivaroxaban-treated group, indicating its coronary artery protection (Mega et al.,
2012).
In this case, acute cerebral infarction is another evidence of arterial embolism, which was present concurrently or subsequently with PE. Cerebral reinfarction was located in the left insular lobe and basal ganglia, accompanied with a partial hemorrhage subsequent to intravenous thrombolysis. It is noted as both an anticoagulation and antiplatelet treatment for patients with arteriovenous embolism. It has been demonstrated that a single antiplatelet drug was associated with a significant reduction in bleeding complications and no increase of thrombotic events in patients taking oral anticoagulant therapy or undergoing percutaneous coronary intervention (Dewilde et al.,
2013). In this case, the patient had accepted short-term triple antithrombotic therapy and then switched to an anticoagulant with an antiplatelet agent for more than one year. During the 16-month follow-up, the quality of life improved without any major clinical bleeding events.
In conclusion, this is the first reported case of PE coincident or concomitant with acute myocardial and cerebral infarction. The anticoagulation and antiplatelet therapy significantly improved the clinical prognosis of arteriovenous embolism in this patient.
Acknowledgements
We thank Dr. Jiong ZHOU from the Department of Neurology of the Second Affiliated Hospital, School of Medicine, Zhejiang University, China, and Dr. Biao JIANG from the Department of Radiology of the Second Affiliated Hospital, School of Medicine, Zhejiang University, China, for their critical reading of the manuscript.
* Project supported by the National Natural Science Foundation of China (Nos. 31171392 and 31371475)Compliance with ethics guidelines Xiao-jie XIE, Ju-bo JIANG, Jun JIIANG, and Jian-an WANG declare that they have no conflict of interest.References
[1] Dewilde, W.J., Oirbans, T., Verheugt, F.W., 2013. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomised, controlled trial.
Lancet, 381(9872):1107-1115.

[2] Goldhaber, S.Z., 2005. Pulmonary thromboembolism. Harrisons Principles of Internal Medicine. McGraw-Hill,New York :1561-1565.

[3] Kumar, V., 2010. Basic Pathology. Elsevier,New Delhi :98
[4] Mega, J.L., Braunwald, E., Wiviott, S.D., 2012. Rivaroxaban in patients with a recent acute coronary syndrome.
N Engl J Med, 366(1):9-19.
[5] Patel, M.R., Mahaffey, K.W., Garg, J., 2011. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation.
N Engl J Med, 365(10):883-891.
[6] Rahimtoola, A., Bergin, J.D., 2005. Acute pulmonary embolism: an update on diagnosis and management.
Curr Probl Cardiol, 30(2):61-114.
[7] Rakhit, R.D., 2003. Case 2: patent foramen ovale (PFO) and paradoxical embolism.
Heart, 89(11):1362
[8] The EINSTEIN Investigators, 2010. Oral rivaroxaban for symptomatic venous thromboembolism.
N Engl J Med, 363(26):2499-2510.
[9] The EINSTEIN-PE Investigators, 2012. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism.
N Engl J Med, 366(14):1287-1297.
[10] Wang, J.A., 2010. Advances in cardiovascular disease: how far is the summit?.
J Zhejiang Univ-Sci B (Biomed & Biotechnol), 11(8):547
[11] Wang, J.A., 2012. Progress and challenges in the cardiovascular field.
J Zhejiang Univ-Sci B (Biomed & Biotechnol), 13(8):587-588.
[12] Yang, Y., Liang, L., Zhai, Z., 2011. Pulmonary embolism incidence and fatality trends in Chinese hospitals from 1997 to 2008: a multicenter registration study.
PLoS ONE, 6(11):e26861
[13] Ying, S.Q., Xiang, M.X., Fang, L., 2010. Temporal changes in circulating P-selectin, plasminogen activator inhibitor-1, magnesium, and creatine kinase after percutaneous coronary intervention.
J Zhejiang Univ-Sci B (Biomed & Biotechnol), 11(8):575-582.
[14] Zhang, S., 2012. Clinical considerations of anticoagulation therapy for patients with atrial fibrillation.
J Zhejiang Univ-Sci B (Biomed & Biotechnol), 13(8):609-615.


Open peer comments: Debate/Discuss/Question/Opinion
<1>