1. Introduction
In kidney transplantation, ischemia-reperfusion injury (IRI) contributes to the allograft dysfunction (Peeters et al.,
2004; Chapman et al.,
2005; Perco et al.,
2007). In native kidneys, IRI is a common cause of acute kidney injury (AKI) in patients who are undergoing cardiac surgery or with critical illness, and it is associated with high mortality and morbidity (Levy et al.,
1996; Schiffl et al.,
2002; Chertow et al.,
2005; Bellomo et al.,
2008; Kellum et al.,
2008; Kinsey et al.,
2008). For decades, non-steroidal anti-inflammatory drugs (NSAIDs) have been used successfully in the treatment of numerous clinical diseases for their anti-inflammatory and analgesic effects. Despite the efficacy, long-term use of NSAIDs could cause renal damage, such as renal papillary necrosis (John and Herzenberg,
2009). Does the short-term and low-dose application of NSAIDs have the same damage, such as patient-controlled analgesia (PCA)?
PCA is usually used for relieving pain after major surgery. NSAIDs are commonly combinated with morphine following major surgery with the aim of reducing morphine’s side-effects (McDaid et al.,
2010). PCA has reduced the morbidity of cardiac, pulmonary, thromboembolic and renal diseases, and also reduced blood loss and transfusion requirements (Kehlet,
2004). However, many animal studies showed that NSAIDs have a protective effect on the IRI, such as heart, lung, and liver (Takeyoshi et al.,
2001; Otani et al.,
2007; Carnieto et al.,
2009). Studies also showed that NSAIDs displayed a renal protective effect after IRI. The patients would take the treatment of NSAIDs for preoperative renal function normally, but NSAIDS can cause renal dysfunction in the early postoperative period. While the treatment was going on, the renal protective effect would occur (Lee et al.,
2007).
Indomethacin (IMT) is one of the most widely used NSAIDs in clinics. An increasing number of studies reported that pretreatment with IMT alone tended to reduce the renal damage after IRI (Schneider et al.,
2009). Feitoza et al. (
2008) showed that pretreatment of mice with 5 mg/kg IMT could protect the renal function and reduce long-term renal fibrosis. The research on rats indicated that low-dose (1 mg/kg) of IMT adopted after ischemia prevented ischemia-induced down-regulation of Oat1/3 during reperfusion and had a significant protective effect on the renal function after AKI (Feitoza et al.,
2002). In this study, we used the mice renal IRI model to evaluate the renoprotection effect of NSAIDs by IMT.
2. Materials and methods
2.1. Animals
Male mice (C57BL/6; 8–10 weeks, 20–24 g) were purchased from Shanghai SLAC Laboratory Animal Co., Ltd., China. All animals were housed individually in standard cages and had free access to a commercial pellet diet and tap water during the study. All procedures were previously reviewed and approved by the internal ethical committee.
2.2. Murine model of renal IRI
All procedures were performed using strict sterile techniques under general anesthesia with pentobarbital sodium (50 mg/kg, intraperitoneal (i.p.) injection). Animals were set on a warming table to maintain a rectal temperature of 37 °C. A midline incision was made and a right nephrectomy performed. A microaneurysm clamp was used to occlude the left renal pedicle for 60 min; the time of ischemia was chosen to obtain a reversible model of ischemic AKI without significant mortality. After the microaneurysm clamp was removed, reperfusion was confirmed visually by the blood flow returning to the kidney. The animals were administered 1 ml of prewarmed (37 °C) sterile saline (i.p.), and the incisions were closed in two layers. The animals were then allowed to recover with free access to food and water. The sham-operated mice underwent dissection of the left renal pedicle without clamping after removal of the right kidney. After 24 h, mice were re-anesthetized, the abdominal cavity was opened, and blood was obtained from inferior vena. The mice were killed and the kidney was harvested, one-half of each was fixed in 10% formalin, and the residual kidney was snap frozen in liquid nitrogen and stored at −80 °C until further processing.
2.3. Study design
After the left renal pedicle was clamped, IMT (Sigma, USA) was administrated i.p. at four doses 1, 3, 5, and 7 mg/kg. Animals were randomly divided into six groups (
n=6):
Sham group: sham+saline;
IRI group (control): IRI+saline;
IRI+1IMT group: IRI+1 mg/kg IMT;
IRI+3IMT group: IRI+3 mg/kg IMT;
IRI+5IMT group: IRI+5 mg/kg IMT;
IRI+7IMT group: IRI+7 mg/kg IMT.
2.4. Renal function
Blood samples (about 0.8 ml) were obtained from each animal at 24 h post-reperfusion and centrifuged at 2000
g for 5 min to obtain the serum. Serum creatinine (SCr) levels were measured as a marker of renal function, using a creatinine kit (Biovision, USA), and analyzed on a microplate reader.
2.5. Serum cytokines
Serum levels of tumor necrosis factor α (TNF-α), interleukin (IL)-6 (Groundwork Biotechnology Diagnosticate, USA), thromboxane B
2 (TxB
2), and 6-keto-prostaglandin F
1α (PGF
1α) (Cayman Chemical Company, USA) were measured using enzyme-linked immunosorbent assay (ELISA) kits according to the manufacturer’s instructions.
2.6. Histological examination
The renal tissues were fixed in 10% neutral buffered formalin for 24 h, and embedded in paraffin, sectioned at 3 μm according to the standard procedure. The sections were deparaffinized and hydrated gradually and then stained with hematoxylin and eosin (H&E). Tissue sections were scored in a blinded manner to evaluate the degree of tubular necrosis as described by Wan et al. (
2011). Tubulointerstitial injury was defined as tubular necrosis, tubular dilatation and/or atrophy, inflammatory cell infiltrate, or cellular edema, and was graded on a scale based on the percentage of tubular affected: 0, normal kidney; 1, minimal necrosis (<5%); 2, mild necrosis (5%–25%); 3, moderate necrosis (25%–75%); 4, severe necrosis (>75%).
2.7. Immunohistochemical staining
Tissues sections of 2-μm thick were dewaxed in xylene and hydrated in graded series of alcohols, and then sections were placed in citrate buffer (pH 6.0) at 120 °C for 10 min. Endogenous peroxidase activity was blocked with 0.3% H
2O
2 for 30 min at room temperature. Non-specific binding was inhibited by incubation for 15 min with normal goat serum. Then, the sections were incubated with primary antibody rabbit anti-mouse against cyclooxygenase (COX)-1 (500× diluted; BioVision) or rabbit anti-mouse against COX-2 (100× diluted; Epitomics) for 60 min at 37 °C. After washing with phosphate buffered saline (PBS), the sections were incubated for 30 min with horse radish peroxidase-conjugated secondary antibody (ChemMate™ EnVision™ Detection kit). The final detection was performed using freshly prepared DAB as a chromogen, and the colorimetric reaction was allowed to proceed for 1 min. The sections were evaluated blindly by counting the labeled cells in triplicate within 40 high-power fields per section.
The intensity of staining was graded as + (weak), ++ (moderate), or +++ (strong), and the number of positive cells was scored as <25%, 26%–50%, or >50% (Miranda et al.,
2000).
2.8. Statistical analyses
All data are expressed as mean±standard error (SE). The Student’s unpaired
t-test was used to compare two groups. All analyses were carried out using the GraphPad Prism 5.0 statistical software package, and
P<0.05 was accepted as statistically significant.
3. Results
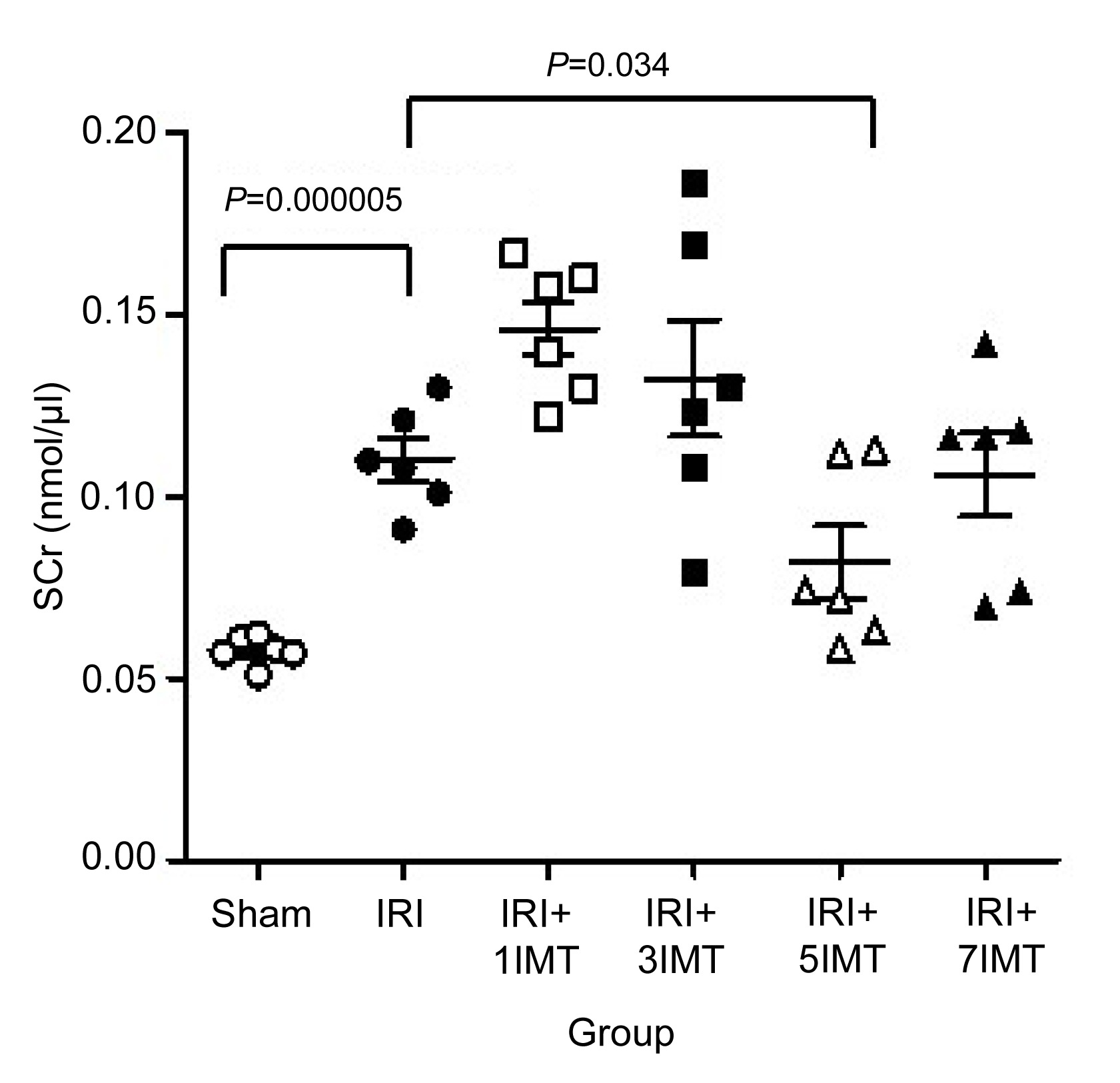
3.1. IMT ameliorates renal dysfunction
We first induced renal IRI models in mice and treated them with IMT or saline as control. By comparison to the sham animals, control animals subjected to renal IRI had apparent increased SCr at 24 h, indicating the acute renal dysfunction (
P=0.000 005) (Fig.
1, Table
1). However, the mice administered with 5 mg/kg IMT after renal IRI had a marked reduction in SCr vs. the IRI group (control) (
P=0.034). The mice administered with 1, 3, 7 mg/kg of IMT had no significant differences in SCr compared with the IRI group.
Fig.1
Effect of IMT on renal dysfunction
The sham group had a lower SCr than the IRI group (P=0.000 005). The 5 mg/kg IMT treatment group (IRI+5IMT) significantly decreased SCr compared to the IRI group (P=0.034). The IRI+1IMT and IRI+3IMT group had higher Scr than the IRI group (P=0.003 and 0.220, respectively). The IRI+7IMT group had no significant differences in Scr compared with the IRI group (P=0.752)
Table 1
Serum creatinine (SCr) after renal IRI
| Group |
SCr* (nmol/μl) |
P value (vs. control) |
| Sham |
0.058±0.004 |
0.000 005 |
| IRI (control) |
0.110±0.013 |
| IRI+1IMT |
0.146±0.036 |
0.003 |
| IRI+3IMT |
0.133±0.039 |
0.220 |
| IRI+5IMT |
0.082±0.024 |
0.034 |
| IRI+7IMT |
0.106±0.028 |
0.752 |
*Data are presented as mean±SE (n=6)
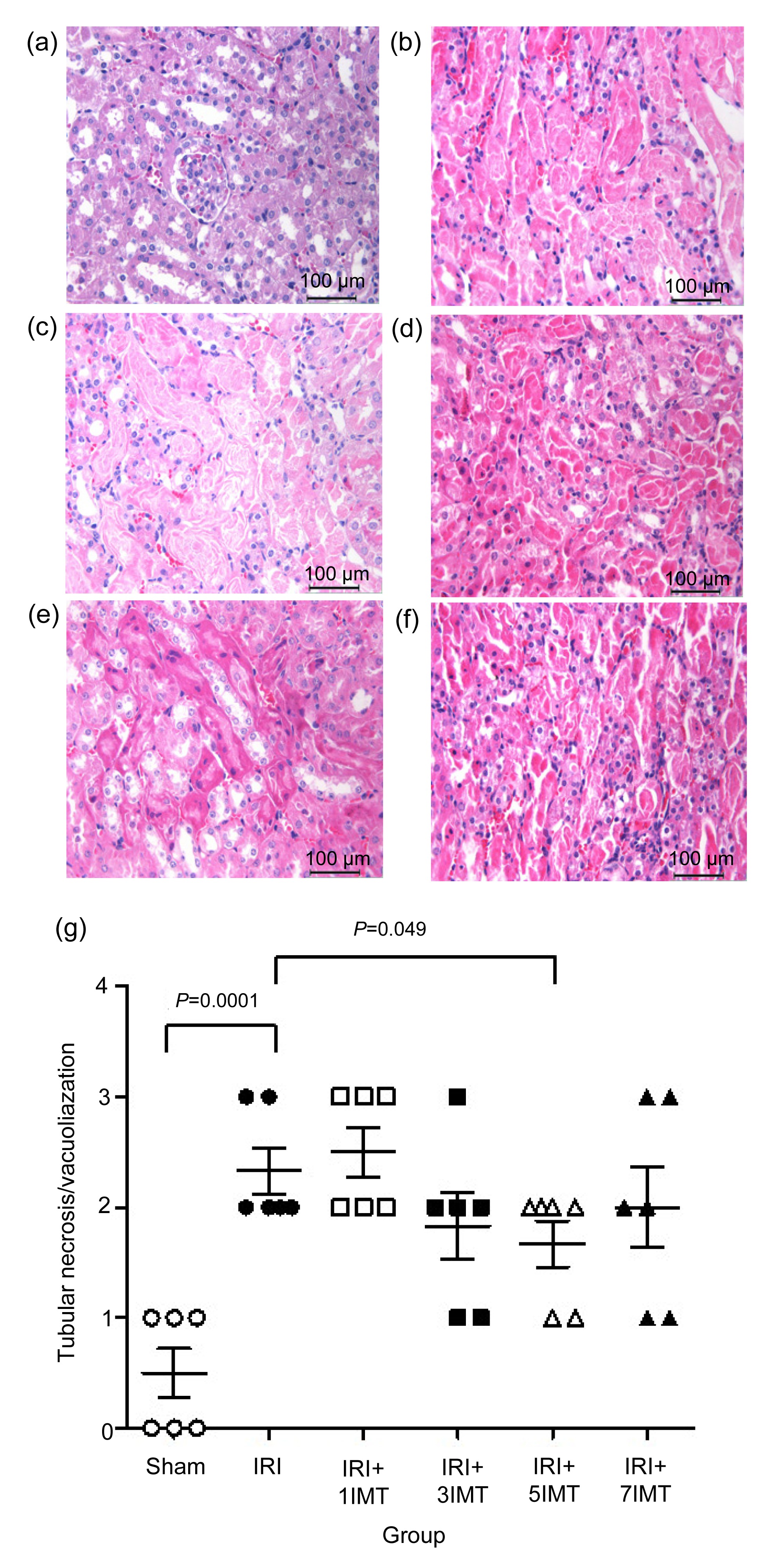
3.2. IMT attenuates the histologic damage
Histology analysis indicated the kidneys from the IRI group had severe tubular injury in the outer medulla, as evidenced by widespread tubular necrosis, luminal congestion, and significant infiltration of neutrophils at 24 h reperfusion. In contrast, renal sections from animals treated with 5 mg/kg IMT showed less tubular injury (Fig.
2e). However, renal sections obtained from animals treated with other doses of IMT (1, 3, 7 mg/kg) showed similar tubular injury as control (Figs.
2c, 2d, and 2f). Quantification of the tubular injury and infiltrating neutrophils in the outer medulla shows a significantly lower mean tubular injury score from the kidneys of mice treated with 5 mg/kg IMT (IRI (2.333±0.516) vs. IRI+5IMT (1.667±0.516),
P=0.049), but no statistically different mean tubular injury score from the kidneys of mice treated with 1, 3, and 7 mg/kg IMT in comparison with the control group (Fig.
2g).
Fig.2
Effects of IMT on histologic damage of mice renal
H&E histopathological section of kidney from sham (a); IRI (b); IRI+1IMT (c); IRI+3IMT (d); IRI+5IMT (e); IRI+7IMT (f). Scores for acute tubular necrosis from six groups (g). The IRI group had a higher scores than the sham group (P=0.0001), IRI+5IMT group had lower scores than the IRI group (P=0.049), and 1, 3, and 7 mg/kg IMT groups had no significant difference compared with the IRI group (P=0.599, 0.209, and 0.448, respectively)
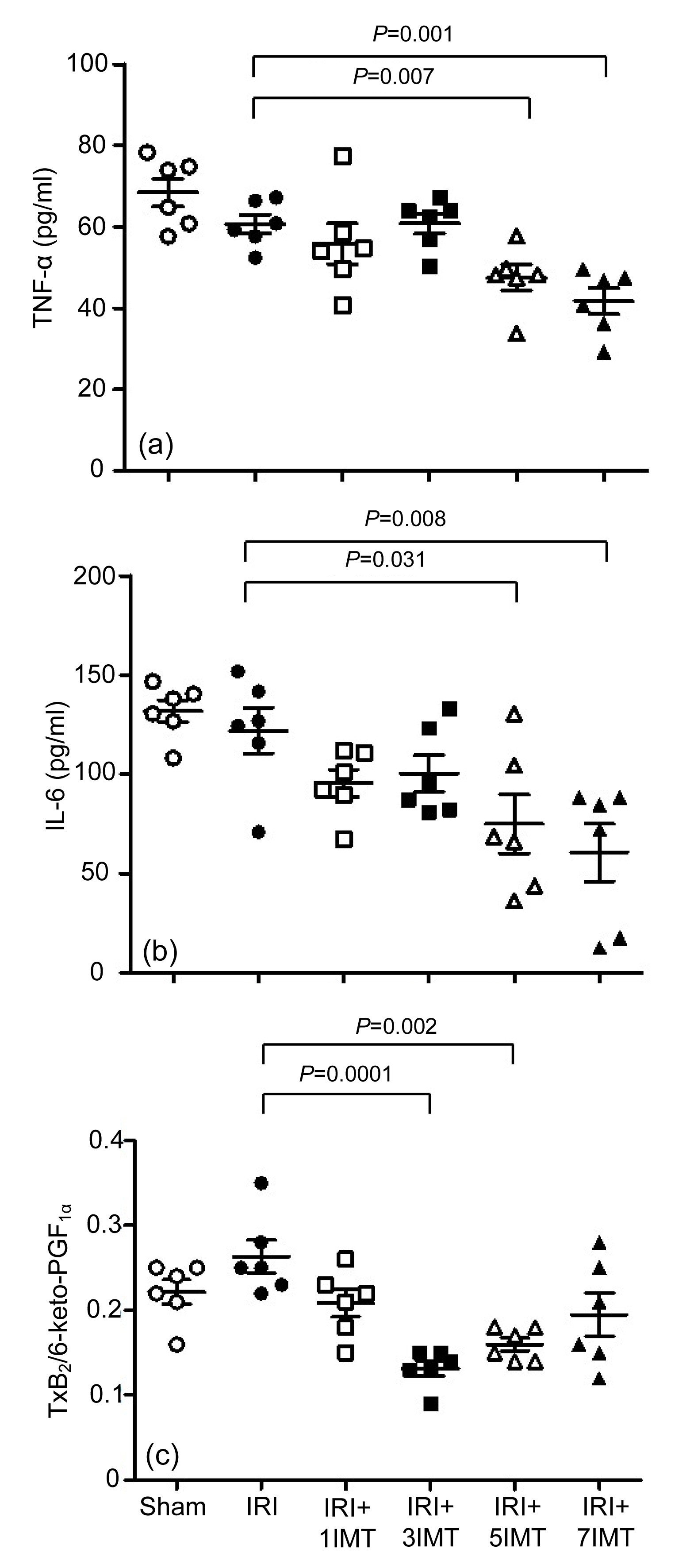
3.3. IMT reduces TNF-α and IL-6 expression levels after renal IRI
It was well known that monocytes/macrophages invading the renal cortical tissue are part of an inflammatory response after ischemia. Thus, the amounts of TNF-α and IL-6 had been determined as markers of renal inflammatory response after ischemia and 24 h reperfusion. Compared with the IRI group, the IMT-treated mice showed significant down-regulation of TNF-α and IL-6 expression levels with the increase in the dose. The mice administered with 5 and 7 mg/kg IMT had a marked reduction in TNF-α activity in renal homogenates: IRI (60.63±5.55) pg/ml vs. IRI+5IMT (47.47±7.69) pg/ml (
P=0.007) and IRI+7IMT (41.65±7.84) pg/ml (
P=0.001) (Fig.
3a, Table
2). A similar result was also detected in the IL-6 activity in serum: IRI (121.96±28.10) pg/ml vs. IRI+5IMT (75.00±36.21) pg/ml (
P=0.031) and IRI+7IMT (60.74±35.76) pg/ml (
P=0.008) (Fig.
3b, Table
2).
Fig.3
Effects of IMT on expression levels of TNF-α (a), IL-6 (b), and TxB2/6-keto-PGF1α (c) after renal IRI
IRI+5IMT and IRI+7IMT groups have significantly lower TNF-α (a) and IL-6 (b) levels than the IRI group; IRI+3IMT and IRI+5IMT groups have lower TxB2/6-keto-PGF1α than the IRI group (c)
Table 2
Effects of IMT on expression levels of TNF-α, IL-6, and TxB2/6-keto-PGF1α after renal IRI
| Group |
TNF-α (pg/ml) |
IL-6 (pg/ml) |
TxB2/6-keto-PGF1α
|
| Sham |
68.380±8.431 |
131.848±13.542 |
0.322±0.034 |
| IRI (control) |
60.627±5.551 |
121.958±28.097 |
0.363±0.047 |
| IRI+1IMT |
55.787±12.216 |
95.465±16.560 |
0.308±0.039 |
| IRI+3IMT |
60.784±6.153 |
100.427±22.310 |
0.232±0.022*
|
| IRI+5IMT |
47.469±7.692*
|
74.998±36.210*
|
0.260±0.019*
|
| IRI+7IMT |
41.652±7.837*
|
60.737±35.755*
|
0.295±0.062 |
*
P<0.05 vs. IRI group
Data are presented as mean±SE (n=6)
3.4. IMT impact on TxB2 and 6-keto-PGF1α expression after renal IRI
Prostanoids have long been known to behave as important physiological and pathological mediators implicated in a number of therapeutic areas of interest. In the kidney, vasodilator prostaglandins (PGI
2, PGE
2, and PGD
2) play an important role in regulating renal blood flow, diminishing vascular resistance, dilating renal vascular beds, and enhancing organ perfusion. On the contrary, thromboxane A
2 (TxA
2) is a vasoconstriction. TxB
2 is a metabolite of TxA
2 and 6-keto-PGF
1α is a metabolite of PGI
2. There is a U-shaped dose-response curve on the ratio of TxB
2 to 6-keto-PGF
1α. Here, the administration of 1 and 7 mg/kg IMT to mice does not significantly improve renal blood flow. The mice administered 3 and 5 mg/kg IMT have a marked reduction in TxB
2/6-keto-PGF
1α: IRI 0.36±0.05 vs. IRI+3IMT 0.23±0.02 (
P=0.0001) and IRI+5IMT 0.26±0.02 (
P=0.002) (Fig.
3c, Table
2).
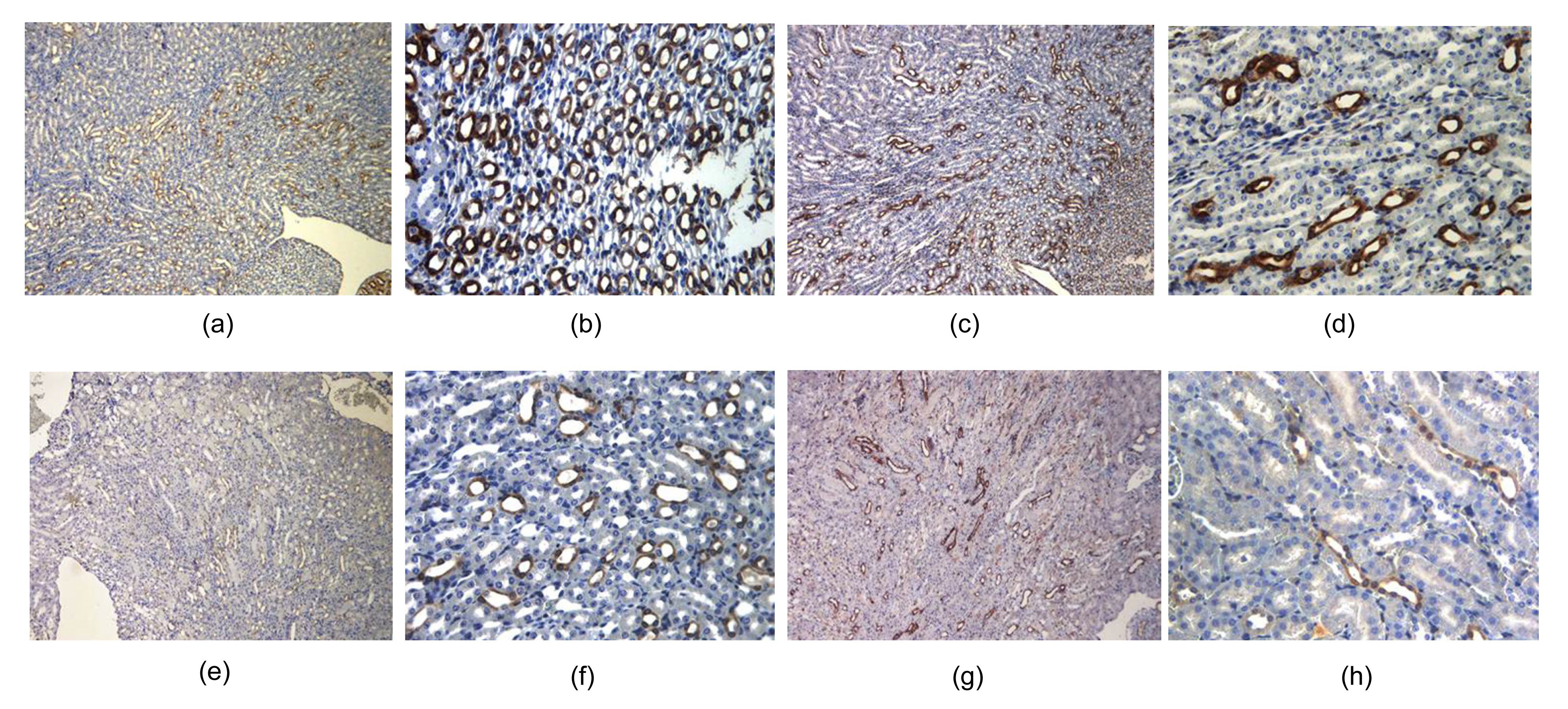
3.5. Immunohistochemical analyses of COX-1 and COX-2
The IRI group had strong COX-1 and COX-2 staining (++–+++) in the renal tubes (number of positive cells >50%; Figs.
4a–4d). For the 5 mg/kg IMT treatment group, COX-1 and COX-2 stainings were low in the renal tubes (number of positive cells <25%), and obviously much lighter (Figs.
4e–4h).
Fig.4
Immunohistochemical analyses of COX-1 and COX-2
(a, b) IRI group had the COX-1 staining (++–+++) in the renal tubes, and the number of positive cells >50%; (c, d) IRI group had the COX-2 staining (++–+++) in the renal tubes, and the number of positive cells >50%; (e, f) 5 mg/kg IMT treatment group had the COX-1 staining (+) in the renal tubes, and the number of positive cells <25%; (g, h) 5 mg/kg IMT treatment group had the COX-2 staining (+) in the renal tubes, and the number of positive cells <25%. (a, c, e, g) Magnification 10×; (b, d, f, h) Magnification 40×
4. Discussion
Previous work on mice indicated that severe dysfunction after renal IRI was ameliorated by treatment with 5 mg/kg IMT i.p. (Feitoza et al.,
2002;
2005). The research on rats showed low-dose (1 mg/kg) IMT had a substantial protective effect on kidney function after AKI (Schneider et al.,
2009). In recent studies, we set 1, 3, 5, and 7 mg/kg IMT treatment in the mice IRI model, and found that 5 mg/kg IMT was the proper dose in this study. It was the direct anti-inflammatory effects of IMT on renal proximal tubular cells, which contributed to the observed protection. And the hemodynamic effect of IMT was also dependent on the appropriate dose, which was due to different sensitivity responses to IMT dosages in different rodent species.
Tissue injury after ischemia was not only caused by hypoxia from interrupted blood supply but also the activated inflammatory response by reperfusion. The peripheral leukocytes recruit and the interstitial cells proliferated in the target tissue (Ysebaert et al.,
2004). An innate immune system was found to be important for the pathogenesis of IRI in recent years. This is mediated by numbers of cytokines/chemokines, adhesion molecules, transcription factors, and other pro-inflammatory factors which were specifically blocked for profound reduction of IRI (Kinsey et al.,
2008; Lutz et al.,
2010). Renal IRI induces inflammatory reactions within the renal parenchyma through increased synthesis of pro-inflammatory cytokines such as IL-1, IL-6, and TNF-α (Feitoza et al.,
2002). TNF-α is a pro-inflammatory cytokine that upregulates its own expression and other cytokines that are pivotal to the inflammatory response (Donnahoo et al.,
1999).
In human and experimental animals, glomerular filtration rate (GFR) reductions had been attributed to persistent vasoconstrictions, potentially contributed to by activation of tubuloglomerular feedback, which was also a result of enhanced delivery of the macula densa solution. Ischemic acute renal failure (ARF) had been referred to as “vasomotor nephropathy” in the past. Post-ischemic kidneys showed increased basal tone and reactivity to vasoconstriction agents, and decreased dilatory responses in arterioles (Bonventre and Weinberg,
2003). The PGE
2 and PGI
2 caused afferent arteriole dilatation and increased GFR, whereas thromboxanes led to constriction (Kinsey et al.,
2008; Lutz et al.,
2010). Maintenance of adequate renal function was dependent on homeostasis of substances, which causes mesangial relaxation and contraction. And this balance is shifted towards vasoconstriction, which was reflected by increased renal vascular resistance and decreased renal blood flow (Furtado et al.,
2008).
Previous researches found that COX-1 and COX-2 participate in acute ischemic injury by evoking endothelial cells oxidative stress (Hamada et al.,
2008; Feitoza et al.,
2010; Talab et al.,
2010). In our study, we found that the acute ischemic injury group had the higher COX-1 and COX-2 expression levels in the kidney. In 5 mg/kg IMT group, the kidney injury was light and the COX-1 and COX-2 expression levels were both lower than those in the IRI group. COX-1 and COX-2 are important for the AKI signaling pathway.
In conclusion, our study highlighted the important role of prophylactic IMT in the response to renal injury in mice. We showed that it involved the modulation of the immune response and renal haemodynamics, and the COX-1 and COX-2 expressions in AKI. Animal studies confirmed the renoprotective effect of IMT at an appropriate dose of 5 mg/kg in mice. There have been no human clinical trials for IMT in human renal IRI based on the consideration of drug safety. Does IMT have a similar effect in humans And what dose is the most appropriate for humans To solve these problems, we need further clinical trails for validation. Therefore, we are calling for more clinical trials to test whether IMT can exert a renoprotective effect during human renal IRI.
* Project supported by the National Key Technology R&D Program of China (No. 2011BAI10B07), the National Basic Research Program (973) of China (No. 2012CB517603), and the National High-Tech R&D Program (863) of China (No. 2012AA02A512)Compliance with ethics guidelines Sheng-hong ZHU, Li-jia ZHOU, Hong JIANG, Rong-jun CHEN, Chuan LIN, Shi FENG, Juan JIN, Jiang-hua CHEN, and Jian-yong WU declare that they have no conflict of interest.References
[1] Bellomo, R., Auriemma, S., Fabbri, A., 2008. The pathophysiology of cardiac surgery-associated acute kidney injury (CSA-AKI).
Int J Artif Organs, 31(2):166-178.

[2] Bonventre, J.V., Weinberg, J.M., 2003. Recent advances in the pathophysiology of ischemic acute renal failure.
J Am Soc Nephrol, 14(8):2199-2210.

[3] Carnieto, A., Dourado, P.M., Luz, P.L., 2009. Selective cyclooxygenase-2 inhibition protects against myocardial damage in experimental acute ischemia.
Clinics, 64(3):245-252.
[4] Chapman, J.R., O'Connell, P.J., Nankivell, B.J., 2005. Chronic renal allograft dysfunction.
J Am Soc Nephrol, 16(10):3015-3126.
[5] Chertow, G.M., Burdick, E., Honour, M., 2005. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients.
J Am Soc Nephrol, 16(11):3365-3370.
[6] Donnahoo, K.K., Meng, X., Ayala, A., 1999. Early kidney TNF-α expression mediates neutrophil infiltration and injury after renal ischemia-reperfusion.
Am J Physiol Regul Integr Comp Physiol, 277(3):R922-R929.
[7] Feitoza, C.Q., Sanders, H., Cenedeze, M., 2002. Pretreatment with indomethacin protects from acute renal failure following ischemia-reperfusion injury.
Transpl Proc, 34(7):2979-2980.
[8] Feitoza, C.Q., Câmara, N.O., Pinheiro, H.S., 2005. Cyclooxygenase 1 and/or 2 blockade ameliorates the renal tissue damage triggered by ischemia and reperfusion injury.
Int Immunopharmacol, 5(1):79-84.
[9] Feitoza, C.Q., Goncalvs, G.M., Semedo, P., 2008. Inhibition of COX1 and 2 prior to renal ischemia/reperfusion injury decreases the development of fibrosis.
Mol Med, 14(11-12):724-730.
[10] Feitoza, C.Q., Semedo, P., Gonalves, G.M., 2010. Modulation of inflammatory response by selective inhibition of cyclooxygenase-1 and cyclooxygenase-2 in acute kidney injury.
Inflamm Res, 59(3):167-175.
[11] Furtado, N., Beier, U.H., Gorla, S.R., 2008. The effect of indomethacin on systemic and renal hemodynamics in neonatal piglets during experimental endotoxemia.
Pediatr Surg Int, 24(8):907-911.
[12] Hamada, T., Tsuchihashi, S., Avanesyan, A., 2008. Cyclooxygenase-2 deficiency enhances Th2 immune responses and impairs neutrophil recruitment in hepatic ischemia/reperfusion injury.
J Immunol, 180(3):1843-1853.
[13] John, R., Herzenberg, A.M., 2009. Renal toxicity of therapeutic drugs.
J Clin Pathol, 62(6):505-515.
[14] Kehlet, H., 2004. Effect of postoperative pain treatment on outcome-current status and future strategies.
Langenbecks Arch Surg, 389(4):244-249.
[15] Kellum, J.A., Bellomo, R., Ronco, C., 2008. Definition and classification of acute kidney injury.
Nephron Clin Pract, 109(4):c182-c187.
[16] Kinsey, G.R., Li, L., Okusa, M.D., 2008. Inflammation in acute kidney injury.
Nephron Exp Nephrol, 109(4):e102-e107.
[17] Lee, A., Cooper, M.C., Craig, J.C., 2007. Effects of nonsteroidal anti-inflammatory drugs on postoperative renal function in adults with normal renal function.
Cochrane Database Syst Rev, (2):CD002765
[18] Levy, E.M., Viscoli, C.M., Horwitz, R.I., 1996. The effect of acute renal failure on mortality. A cohort analysis.
JAMA, 275(19):1489-1494.
[19] Lutz, J., Thrmel, K., Heemann, U., 2010. Anti-inflammatory treatment strategies for ischemia/reperfusion injury in transplantation.
J Inflamm, 7:27
[20] McDaid, C., Maund, E., Rice, S., 2010. Paracetamol and selective and non-selective non-steroidal anti-inflammatory drugs (NSAIDs) for the reduction of morphine-related side effects after major surgery: a systematic review.
Health Technol Assess, 14(17):1-153.
[21] Miranda, R.N., Briggs, R.C., Kinney, M.C., 2000. Immunohistochemical detection of cyclin D1 using optimized conditions is highly specific for mantle cell lymphoma and hairy cell leukemia.
Modern Pathol, 13(12):1308-1314.
[22] Otani, Y., Takeyoshi, I., Yoshinari, D., 2007. Effects of the COX-2 inhibitor FK3311 on ischemia—reperfusion injury in the rat lung.
J Invest Surg, 20(3):175-180.
[23] Peeters, P., Terryn, W., Vanholder, R., 2004. Delayed graft function in renal transplantation.
Curr Opin Crit Care, 10(6):489-498.
[24] Perco, P., Pleban, C., Kainz, A., 2007. Gene expression and biomarkers in renal transplant ischemia reperfusion injury.
Transpl Int, 20(1):2-11.
[25] Schiffl, H., Lang, S.M., Fischer, R., 2002. Daily hemodialysis and the outcome of acute renal failure.
N Engl J Med, 346(5):305-310.
[26] Schneider, R., Meusel, M., Renker, S., 2009. Low-dose indomethacin after ischemic acute kidney injury prevents downregulation of Oat1/3 and improves renal outcome.
Am J Physiol Renal Physiol, 297(6):F1614-F1621.
[27] Takeyoshi, I., Sunose, Y., Iwazaki, S., 2001. The effect of a selective cyclooxygenase-2 inhibitor in extended liver resection with ischemia in dogs.
J Surg Res, 100(1):25-31.
[28] Talab, S.S., Emami, H., Elmi, A., 2010. Chronic lithium treatment protects the rat kidney againest ischemia/reperfusion injury: the role of nitric oxide and cyclooxygenase pathways.
Eur J Pharmacol, 647(1-3):171-177.
[29] Wan, X., Fan, L., Hu, B., 2011. Small interfering RNA targeting IKKβ prevents renal ischemia-reperfusion injury in rats.
Am J Physiol Renal Physiol, 300(4):F857-F863.
[30] Ysebaert, D.K., de Greef, K.E., de Beuf, A., 2004. T cells as mediators in renal ischemia/reperfusion injury.
Kidney Int, 66(2):491-496.

Open peer comments: Debate/Discuss/Question/Opinion
<1>