1. Introduction
Differentiated thyroid carcinoma (DTC) is a common malignancy and usually has a good prognosis. Bone metastasis is rare in DTC with an incidence of about 5.5% (Bernier et al.,
2001). It may cause severe complications and lead to poorer prognosis and shorter life expectancy (Sugino et al.,
2014). However, the treatment of DTC with bone metastasis is still controversial. Surgery or radioiodine therapy alone is usually unsatisfactory, and thus the management needs multidisciplinary collaboration. The current study shows a patient diagnosed as thyroid carcinoma with spinal metastasis, who was treated in December 2012. In addition, 11 cases were reviewed to analyze and discuss the diagnosis and treatment of DTC with bone metastasis.
2. Case report
A 65 year-old female was admitted to the General Surgery Department of the Second Affiliated Hospital, Zhejiang University (Hangzhou, China) in December 2012, presenting with a complaint of the progressive swelling of her neck for two years, denying sweating, palpitations, agitation, bulimia, pain, dyspnea, hoarseness, or dysphagia, which may be caused by the huge tumor. She had a history of hypertension and diabetes mellitus. Contrast-enhanced neck computed tomography (CT) scans and magnetic resonance image (MRI) revealed the lesions in the 6th cervical vertebra body and left processus transversus (Fig.
1). Her serum thyroid-stimulating hormone (TSH) was normal and thyroglobulin (Tg) was 915.3 ng/ml (reference range: 1.4–78.0 ng/ml).
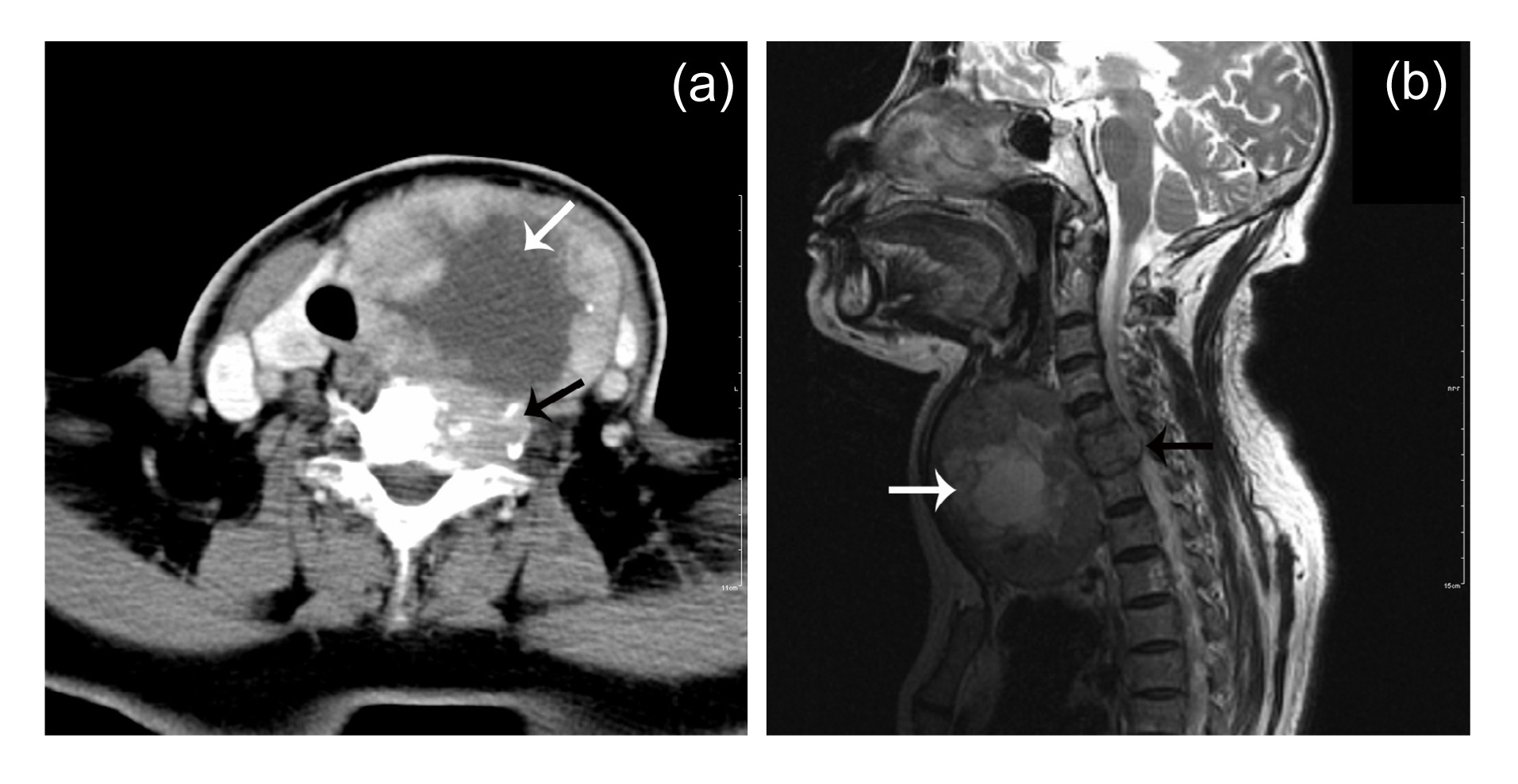
Fig.1
Contrast-enhanced CT and MRI image examinations of the patient in present case
(a) The contrast-enhanced CT demonstrated a 7 cm×8.6 cm sized tumor in the left lobe of the thyroid gland with hypodense in the center (white arrow). Osteolytic destruction could be detected on the 6th cervical vertebra body and left processus transversus (black arrow). (b) MRI sagittal T2-weighted images showed enlarged thyroid lobe (white arrow) and that the 6th cervical vertebra body was invaded, oppressing the spinal cord (black arrow)
The patient was treated with total thyroidectomy, levels II–VI lymph node dissections, cervical corpectomy, and internal fixation, followed by hormone replacement therapy and radioiodine therapy. During the operation, multiple nodules were detected on both lobes and the ones in the left lobe fused to a mass, with a diameter of 8 cm (Fig.
2a). Levels II–VI lymph nodes were detected. The 6th cervical vertebra body was seriously damaged, oppressing the spinal cord. The thyroidectomy and lymph node dissection were conducted successfully. Levels II–VI lymph nodes were dissected. Diskectomy was performed between C5 and C6, C6 and C7 followed by the corpectomy on the 6th cervical vertebra. A titanium mesh (SYNTHES) filled with bone cement was used for the reconstruction and the spine was stabilized with an anterior cervical screw-plate fixation system (SYNTHES) (Fig.
2b). Pathological examination confirmed that follicular thyroid carcinoma and the lesions on C6 were metastatic thyroid carcinoma.
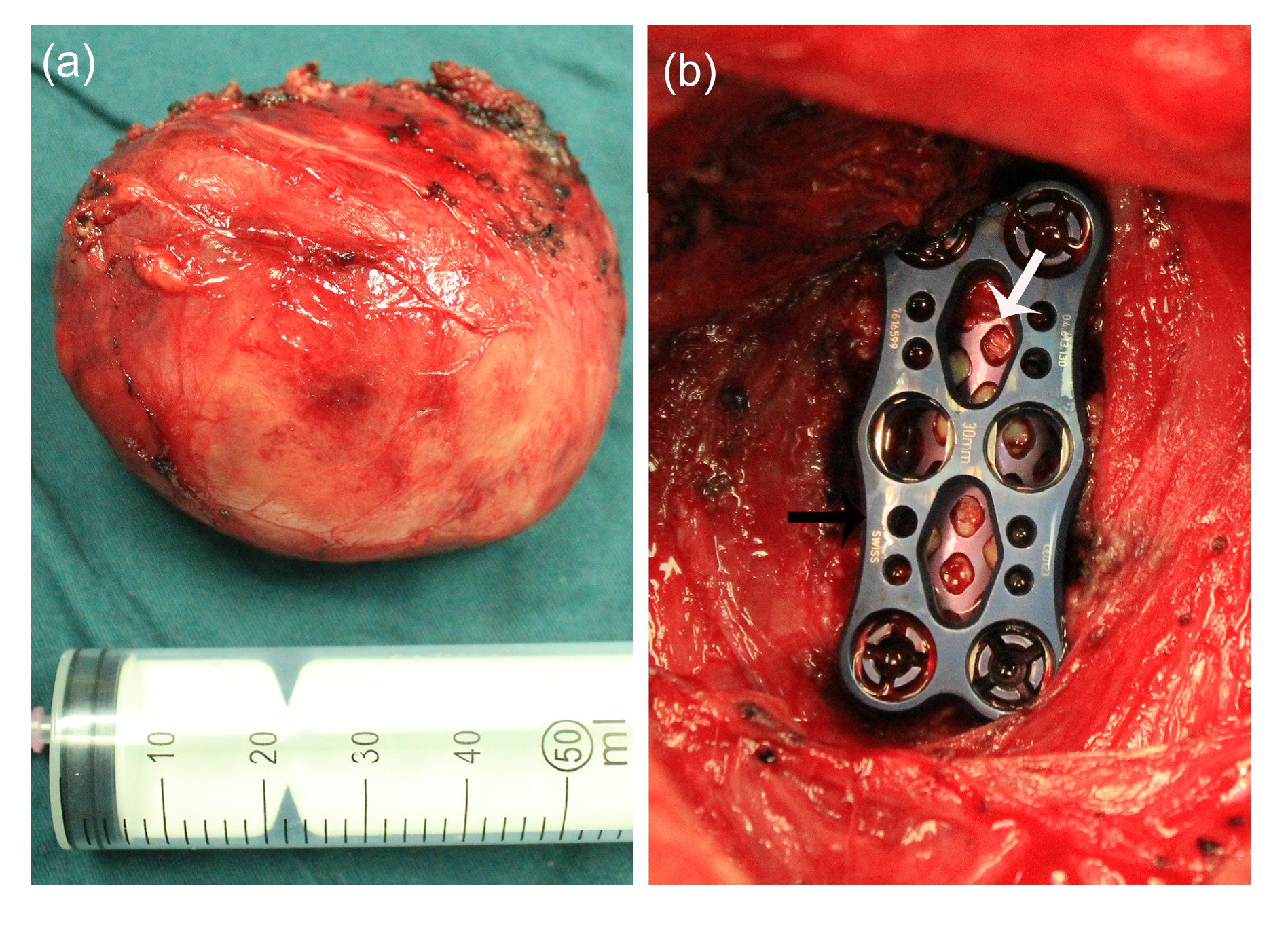
Fig.2
Gross specimen and internal fixation
(a) The gross specimen of the left lobe. Nodules fused to a mass, with a diameter of 8 cm. The tumor invaded outside the membrane. The trachea and the esophagus are not invaded. (b) A titanium mesh (SYNTHES) (black arrow) filled with bone cement was used to finish the reconstruction and the spine was stabilized with an anterior cervical screw-plate fixation system (SYNTHES) (white arrow)
After the surgery, the patient took thyroid hormone replacement therapy (L-T4 100 μg/d) and the TSH concentration was controlled under 0.1 mU/L. Three months later, the patient took I
131 adjuvant therapy, with a dose of 3.7 GBq (100 mCi) and nine months later for the second time with the same dose. A 15-month follow-up was conducted with no evidence of recurrence.
3. Literature review
The Chinese Biology and Medicine Database (
http://sinomed.imicams.ac.cn/zh), the Chinese Periodical Database of Science and Technology (
http://lib.cqvip.com), and the China Hospital Knowledge Database (
http://www.chkd.cnke.net) were searched for the cases of thyroid carcinoma with bone metastasis between January 1996 and December 2013 and 11 cases from five Chinese articles were identified (Table
1).
Table 1
Clinical data of 12 cases of thyroid carcinoma with bone metastasis
| Case |
Age (year) |
Gender |
Thyroid carcinoma histology |
Surgery on primary site |
Symptom of metastasis |
Location of metastasis |
Intervention for bone metastasis |
Outcome, follow-up |
| Chen et al., 2013
|
48 |
Female |
Follicular |
Total thyroidectomy |
Acroanesthesia, left jaw pain, difficulty in opening mouth |
Cervical vertebra, lumbar vertebra, mandible |
Metastasectomy+cervical vertebra internal fixation |
Not available |
| Si and Guan, 2007
|
43 |
Male |
Papillary |
Unilateral lobectomy |
Asymptomatic |
Rib, scapula, cervical vertebra, lung |
Chemotherapy |
Died of metastatic carcinoma recurrence, 52 months |
| Si and Guan, 2007
|
72 |
Female |
Papillary |
Near-total thyroidectomy |
Right crotch pain |
Right ilium |
No intervention |
Died of unknown reason, 7 d |
| Si and Guan, 2007
|
53 |
Male |
Follicular |
Unilateral lobectomy |
Asymptomatic |
Caput fibulae, Rib, ilium, lung |
Caput fibulae tumor curettage |
Died of metastatic carcinoma recurrence, 28 months |
| Si and Guan, 2007
|
42 |
Female |
Papillary |
Total thyroidectomy |
Chest pain |
Rib, lung |
I131 adjuvant therapy |
No recurrence, 42 months |
| Si and Guan, 2007
|
56 |
Female |
Papillary |
Total thyroidectomy |
Pain in waist and lower extremities |
Lumbar vertebra |
Metastasectomy, lumbar vertebra internal fixation+I131 adjuvant therapy |
No recurrence, 2 months |
| Ao and Dong, 1998
|
59 |
Male |
Follicular |
No intervention |
Rib pain |
Rib |
Metastasectomy |
Died of multiple organ metastasis, 7 years |
| Ao and Dong, 1998
|
50 |
Female |
Follicular |
No intervention |
Lumbago, mobility limitation |
Lumbar vertebra |
Metastasectomy+internal fixation |
No recurrence, 20 d |
| Hu et al., 2003
|
46 |
Male |
Follicular |
Lobectomy |
Left tempora pain |
Right ossa temporale |
Metastasectomy |
Not available |
| Hu et al., 2003
|
65 |
Female |
Follicular |
Total thyroidectomy |
Occipitalia pain |
Occipital bone |
Metastasectomy |
Not available |
| Chen et al., 1996
|
48 |
Female |
Papillary |
No intervention |
Lumbosacral portion pain, both lower extremities numbness |
Lumbar vertebra |
Vertebraectomy, vertebral body replacement |
Not available |
| Present |
65 |
Female |
Follicular |
Total thyroidectomy |
Asymptomatic |
Cervical vertebra |
Metastasectomy+cervical vertebra internal fixation+I131 adjuvant therapy |
No recurrence, 15 months |
The mean age of the 12 patients at presentation was (53.9±9.2) years (range, 42–72 years) and the male to female ratio was 1:2. All the cases were diagnosed with DTC, of which seven were follicular thyroid carcinoma and others were papillary carcinoma. Nine cases received total/near-total thyroidectomy or lobectomy while the other three patients refused for personal reasons. As for the metastatic site, the most common one was the spine (6/12), followed by the rib (4/12). Additional sites such as ilium (2/12), skull (2/12), mandible (1/12), and caput fibulae (1/12) were also reported. Nine cases had symptoms including pain, numbness, and mobility limitation. Numbness and mobility limitation occurred in the cases with spinal metastasis, which were caused by the oppressed spinal cord. Carcinoma also invaded the lung in three cases besides metastasizing to the bone. The intervention for bone metastasis was one-stage operation (9/12), I
131 adjuvant therapy (3/12), chemotherapy (1/12), and no intervention (1/12). The follow-up date ranged from 7 d to 7 years, with four cases remaining unavailable. In the other eight cases treated by on-stage surgery, seven cases received metastasectomy including our patient.
4. Discussion
Thyroid carcinoma constitutes 1% of all malignancies, 0.5% in men and 1.5% in women (Ramadan et al.,
2012). Distant metastases are detected in 10%–15% of patients diagnosed with differentiated thyroid cancer (Muresan et al.,
2008), leading to poorer prognosis and shorter life expectancy (Sugino et al.,
2014). Bone metastases from thyroid carcinoma may cause severe complications and the management needs multidisciplinary cooperation. However, specialized general surgeons may ignore the symptoms reflecting the bone metastasis, which often leads to the misdiagnosis. Moreover, the treatment is still controversial and the outcome is usually unsatisfactory.
Thorough pre-operative examinations are the basic foundation for accurate diagnosis and favorable prognosis. The examination for thyroid carcinoma has been well reported. There is a series of pre-operative examinations to diagnose metastasis from thyroid carcinoma. CT of the neck and chest and MRI of the spine, pelvis, and femurs can be useful to visualize metastatic foci (Baudin and Schlumberger,
2007). Scintigraphy-scan of bone and positron emission tomography (PET)-CT can be applied to investigate further skeletal metastases for tumor staging (Delank et al.,
2011).
Surgical resection has remained the first choice for the treatment of DTC (Venkat and Guerrero,
2013). Total/near-total thyroidectomy and thyroid lobectomy are the two most accepted options (Venkat and Guerrero,
2013). In the present case and eleven reviewed cases, nine cases received total/near-total thyroidectomy or lobectomy, while the other three patients refused for personal reasons. Total/near-total thyroidectomy is recommended for patients with papillary thyroid carcinoma greater than or equal to 1 cm, as well as those smaller than 1 cm in size while there is nodular disease involving the contralateral lobe, regional or distant metastases, a personal history of head and neck radiation, or a family history of thyroid carcinoma. As for patients with follicular thyroid carcinoma, patients with a history of head or neck radiation or nodular disease involving the contralateral lobe of the thyroid gland should receive a total thyroidectomy (Jin et al.,
2013). Metastases in lymph nodes are risk factors of increasing of recurrence and death rates (Zaydfudim et al.,
2008). The consensus has been reached in guidelines that central neck lymph node dissection (CNLD) should be performed on patients with clinically evident (cN1 a) level VI lymph nodes (Sosa,
2013).
Resection of solitary bone metastasis, together with total thyroidectomy, could increase survival rate (Pasupula et al.,
2012). Wu et al. (
2008), who analyzed 44 patients of thyroid carcinoma with bone metastasis, showed that proper operations aiming at preventing or treating complications of metastatic bone disease appear to be useful in improving morbidity in patients with skeletal disease. Bernier et al. (
2001) retrospectively studied 109 DTC with bone metastasis, in which 24 (22%) patients were treated by complete excision of the metastasis, 60 (55%) patients were treated by partial removal, while others did not receive any surgery, with the median survival time being 6.2, 4.2, and 2.5 years, respectively (
P<0.05). The indications for the surgical intervention on bone metastasis are as follows: (1) continuous pain; (2) solitary bone metastasis; (3) insensitivity to other treatment; (4) existence or high risk factors of pathologic fracture and paraplegia; (5) obvious manifestation of neurothlipsis (Ramadan et al.,
2012). Meanwhile, multiple organ metastasis and poor general condition are regarded as the contraindications for surgery. In the present study and eleven reviewed cases, nine patients received one-stage operation on the metastatic site. The operation methods normally include curative surgery, aiming at removing the whole tumor, and palliative surgery, which only alleviates physical pain and relieves neural compression. As for spinal metastasis, curative surgery is debulking surgery or total en bloc surgery, followed by internal fixation. Palliative surgery is only to relieve the compression on the spinal cord. In our experience, curative surgery should be conducted on patients with a solitary bone metastasis who are in good general condition and have a long expectation of life. The patients with multiple metastases are often in the advanced stage, which is almost impossible to cure by surgery. Thus, the leading surgical treatment is palliative surgery. Thus, we should weigh the advantages and disadvantages between efficacy and complications to decide whether the patients should have surgery and determine what kind of surgery should be conducted. Additionally, scoring systems can be applied to help choose the therapy type, among which the most famous are Tomita scoring system (Tomita et al.,
2001) and Tokuhashi scoring system (Tokuhashi et al.,
2005).
Adjuvant therapy can prolong survival and improve quality of life by elimination of microscopic residual or metastatic disease after surgery (Sherma,
2003). In a study of 106 cases, Qiu et al. (
2011) pointed out that radioiodine therapy could significantly decrease or at least stabilize serum Tg level as well as alleviate pain on the bone. It could also help shrink or stabilize lesions for most DTC patients with bone metastasis. Petrich et al. (
2001) also conducted a retrospective study of 107 patients, with the conclusion that bone metastases from DTC could be treated by radioiodine therapy, despite the contrary opinion that bone metastases had general resistance to I
131 therapy (Schlumberger et al.,
1996). The dose of I
131 should be 3.7–5.5 GBq for an adult and 37 MBq/kg for a child (Klain et al.,
2002). However, the optimal doses are still under investigation.
Thyroid hormone replacement therapy should be given in order to rectify the resulting hypothyroidism and increase the survival rate. It is indicated that with high doses of replacement therapy, the recurrence of the cancer decreased (Ramadan et al.,
2012). When TSH is >2 mU/L, the mortality and recurrence increase (Hovens et al.,
2007). However, long-term usage of thyroid hormone above physical dosage will lead to sub-clinical hyperthyreosis. The ideal aim of thyroid hormone replacement therapy is reducing the mortality and recurrence, simultaneously avoiding side effects. It is mandatory to evaluate the thyroid function periodically. Our patient took L-T4 100 μg/d and received the appropriate effect.
The application of radiation is still controversial. Proye et al. (
1992) retrospectively analyzed 28 patients with radiation, in which 23 received complete response. However, Bernier et al. (
2001) reported 109 DTC cases with bone metastasis, in which 39 received radiation and 70 not, with the median survival time being 4.3 and 3.8 years, respectively. However, the median survival time turned out to have no significant differences. In our department, radiation is not generally used in patients with DTC, as well as the reviewed patients. Thus, more researches are needed to evaluate the function of radiation.
Bisphosphonates have been affirmed to be highly effective in avoiding bone resorption and pathologic fracture, and reducing local recurrence (Zhang et al.,
2013). Preliminary studies have suggested that bisphosphonates may prevent cancer-treatment-induced bone loss because of reduced estrogenic signaling caused by hormone therapy (Santini et al.,
2006). The study of Orita et al. (
2011) consisted of 50 patients with bone metastases from DTC treated at the Cancer Institute Hospital of Tokyo (Japan), in which 28 patients without bisphosphonate therapy were defined as Group A and 22 patients with bisphosphonates therapy were defined as Group B. The result was that bone fracture, spinal cord compression, and hypercalcemia occurrence were significantly lower in Group B (3 of 22 patients, 14%) than in Group A (14 of 28 patients, 50%), with
P=0.007, which proves the effect of bisphosphonates.
5. Conclusions
DTC with bone metastasis significantly decreases survival rate. A thorough pre-operative examination is crucial to evaluate the tumor stage and discover the metastasis. The treatment needs multidisciplinary cooperation. Surgical resection is still the first choice for cure, while combined one-stage surgery on the primary and metastatic sites followed by hormone replacement therapy and radioiodine therapy is an applicable treatment. More researches are needed to evaluate the function of radiation.
* Project supported by the National Natural Science Foundation of China (No. 81101837)Compliance with ethics guidelines Wei-dong ZHANG, Da-ren LIU, Cheng-cheng FENG, Chuan-biao ZHOU, Chen-ni ZHAN, Ri-sheng QUE, and Li CHEN declare that they have no conflict of interest.References
[1] Ao, Y.Z., Dong, S., 1998. Bone metastasis revealed thyroid carcinoma: 2 cases.
Chin J Clin Oncol, (in Chinese),25(6):53
[2] Baudin, E., Schlumberger, M., 2007. New therapeutic approaches for metastatic thyroid carcinoma.
Lancet Oncol, 8(2):148-156.


[3] Bernier, M.O., Leenhardt, L., Hoang, C., 2001. Survival and therapeutic modalities in patients with bone metastases of differentiated thyroid carcinomas.
J Clin Endocrinol Metab, 86(4):1568-1573.
[4] Chen, Z.H., Huang, T.Q., Li, W., 2013. Metastatic follicular thyroid carcinoma to the mandible: a case report and literature review.
J Dent Prev Treat, (in Chinese),21(10):535-539.
[5] Chen, Z.Q., Wang, X., Xing, J.L., 1996. Lumbar vertebral body revealed thyroid carcinoma: a case report.
Orthop J China, (in Chinese),4(3):234
[6] Delank, K.S., Wendtner, C., Eich, H.T., 2011. The treatment of spinal metastases.
Dtsch Arztebl Int, (in German),108(5):71-79.
[7] Hovens, G.C., Stokkel, M.P., Kievit, J., 2007. Associations of serum thyrotropin concentrations with recurrence and death in differentiated thyroid cancer.
J Clin Endocrinol Metab, 92(7):2610-2615.
[8] Hu, S., Pei, Y.E., Zhu, Y.J., 2003. Thyroid carcinoma with skull metastasis: 2 cases.
Chin J Clin Neurosurg, (in Chinese),8(2):47
[9] Jin, J., Phitayakorn, R., Wilhelm, S.M., 2013. Advances in management of thyroid cancer.
Curr Probl Surg, 50(6):241-289.
[10] Klain, M., Ricard, M., Leboulleux, S., 2002. Radioiodine therapy for papillary and follicular thyroid carcinoma.
Eur J Nucl Med Mol Imaging, 29(S2):S479-S485.
[11] Muresan, M.M., Olivier, P., Leclere, J., 2008. Bone metastases from differentiated thyroid carcinoma.
Endocr Relat Cancer, 15(1):37-49.
[12] Orita, Y., Sugitani, I., Toda, K., 2011. Zoledronic acid in the treatment of bone metastases from differentiated thyroid carcinoma.
Thyroid, 21(1):31-35.
[13] Pasupula, A.P., Dorankula, S.P., Thokala, M.R., 2012. Metastatic follicular thyroid carcinoma to the mandible.
Indian J Dent Res, 23(6):843
[14] Petrich, T., Widjaja, A., Musholt, T.J., 2001. Outcome after radioiodine therapy in 107 patients with differentiated thyroid carcinoma and initial bone metastases: side-effects and influence of age.
Eur J Nucl Med, 28(2):203-208.
[15] Proye, C.A., Dromer, D.H., Carnaille, B.M., 1992. Is it still worthwhile to treat bone metastases from differentiated thyroid carcinoma with radioactive iodine?.
World J Surg, 16(4):640-645.
[16] Qiu, Z.L., Song, H.J., Xu, Y.H., 2011. Efficacy and survival analysis of
131I therapy for bone metastases from differentiated thyroid cancer.
J Clin Endocrinol Metab, 96(10):3078-3086.
[17] Ramadan, S., Ugas, M.A., Berwick, R.J., 2012. Spinal metastasis in thyroid cancer.
Head Neck Oncol, 4(1):39
[18] Santini, D., Fratto, M.E., Vincenzi, B., 2006. Zoledronic acid in the management of metastatic bone disease.
Expert Opin Biol Ther, 6(12):1333-1348.
[19] Schlumberger, M., Challeton, C., de Vathaire, F., 1996. Radioactive iodine treatment and external radiotherapy for lung and bone metastases from thyroid carcinoma.
J Nucl Med, 37(4):598-605.
[20] Sherma, S.I., 2003. Thyroid carcinoma.
Lancet, 361(9356):501-511.
[21] Si, C., Guan, M., 2007. Differentiated thyroid carcinoma with bone metastasis: analysis of 5 cases.
Mod J Integr Tradit Chin West Medline, (in Chinese),16(22):3196-3197.
[22] Sosa, J.A., 2013. Is routine prophylactic central neck dissection indicated for low-risk papillary thyroid cancer: can we determine cost-effectiveness if we are unsure about its effectiveness and safety?.
Surgery, 154(6):1146-1147.
[23] Sugino, K., Kameyama, K., Nagahama, M., 2014. Follicular thyroid carcinoma with distant metastasis: outcome and prognostic factor.
Endocr J, 61(3):273-279.
[24] Tokuhashi, Y., Matsuzaki, H., Oda, H., 2005. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis.
Spine, 30(19):2186-2191.
[25] Tomita, K., Kawahara, N., Kobayashi, T., 2001. Surgical strategy for spinal metastases.
Spine, 26(3):298-306.
[26] Venkat, R., Guerrero, M.A., 2013. Recent advances in the surgical treatment of differentiated thyroid cancer: a comprehensive review.
Sci World J, 2013:425136
[27] Wu, K., Hou, S.M., Huang, T.S., 2008. Thyroid carcinoma with bone metastases: a prognostic factor study.
Clin Med Oncol, 2:129-134.
[28] Zaydfudim, V., Feurer, I.D., Griffin, M.R., 2008. The impact of lymph node involvement on survival in patients with papillary and follicular thyroid carcinoma.
Surgery, 144(6):1070-1078.
[29] Zhang, D., Yin, H., Wu, Z., 2013. Surgery and survival outcomes of 22 patients with epidural spinal cord compression caused by thyroid tumor spinal metastases.
Eur Spine J, 22(3):569-576.
 ORCID:
ORCID: 
Open peer comments: Debate/Discuss/Question/Opinion
<1>